BackgroundDespite well-characterised effects of smoking and alcohol on bone health in older adults, evidence remains limited regarding their impact on bone quality during peak bone mass acquisition in young adults (18–30 years).
ObjectivesAnalysing the relationship between bone quality, alcohol consumption and smoking, considering physical activity (PA) and body composition.
Sample and methodsThe sample consisted of 1001 Slovak men and women aged 18–30 years (mean age, 22±2.35 years). Bone quality was measured using a quantitative ultrasound device (Sunlight MiniOmni™), which yielded Z-score data. Body composition variables, including skeletal muscle mass (SMM; kg) and per cent body fat (PBF; %), were assessed using a bioimpedance analyser (InBody 770). Additional behavioural factors, including alcohol consumption, smoking and PA, were collected using the WHO STEPS 2014 questionnaire.
ResultsIn the regression analysis, duration of alcohol consumption positively predicted bone quality Z-scores (standardised beta equals 0.172, 95% CI [0.03, 0.10], p is less than 0.001), while cigarette smoking quantity was negatively associated (standardised beta equals minus 0.113, 95% CI [−0.01, −0.00], p equals 0.042). The SNHA confirmed the findings of the previous analysis concerning alcohol (r equals 0.19). Conversely, for smoking (r equals 0.23), it identified an inverse relationship, noting a positive effect on bone health, a finding likely mediated by the association with alcohol consumption.
ConclusionLifestyle risk factors, including smoking and alcohol consumption, are associated with bone tissue quality in young adults; however, due to the mixed results available in the literature and in our study, future studies are required.
Keywords: Bone health, Alcohol consumption, Smoking, Young adults
Conflict of Interest: The authors report no conflicts of interest.
Citation: Sulis, S. et al. (2026). Association between alcohol consumption, smoking and bone tissue quality in Slovak young adults assessed by radial quantitative ultrasound . Human Biology and Public Health. https://doi.org/10.52905/hbph2026.112.
Permissions: The copyright remains with the authors. Copyright year 2026. Unless otherwise indicated, this work is licensed under a Creative Commons License Attribution 4.0 International. This does not apply to quoted content and works based on other permissions.
Alcohol consumption and smoking influence bone tissue in young adults. Although smoking and high alcohol consumption are linked to lower bone density, no direct causal relationship has been found. Recognising these factors early may help guide strategies for preventing future bone health issues. Further research on the effects of alcohol and smoking is needed.
Abbreviations
ACAlcohol consumers
BMDBone mineral density
BMIBody mass index
CmaxPeak blood alcohol concentration
DAGDirected acyclic graph
DBPDiastolic blood pressure
FDRFalse discovery rate
NESARCNational Epidemiologic Survey on Alcohol and Related Conditions
OPGOsteoprotegerin
PAPhysical activity
PBFPer cent body fat
QUSQuantitative ultrasound
RANKLReceptor activator of nuclear factor-kappa B ligand
SBPSystolic blood pressure
SMMSkeletal muscle mass
SNHASt. Nicolas House Analysis
SOSspeed of sound
WHOWorld Health Organisation
WHRWaist-to-hip ratio
WHtRWaist-to-height ratio
Contents
Funding statement
Ministry of Education, Science, Research and Sport of the Slovak Republic (KEGA 046UK-4/2023) and by Comenius University Bratislava (UK/1007/2025; Grant project title: Energy drinks and eating habits impact on peripheral skeletal quality and health in early adulthood).
Introduction
Alcohol and smoking prevalence in young adults
Several significant trends and associations are found on the prevalence of alcohol consumption and smoking among young adults; moreover, these behaviours are prevalent in this demographic and often occur concomitantly. According to a study utilising data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), approximately 25% of young adults (aged 18–25) are current smokers, with 7% engaging in non-daily smoking. In the same group, 71% were current consumers, 39% reported binge-drinking at least once a month and 41% met the criteria for hazardous alcohol consumption, with 18% having alcohol use disorders. This study underscores a strong association between smoking status and alcohol use patterns, with daily smokers exhibiting more pronounced alcohol use behaviours than non-daily smokers or non-smokers (Harrison et al. 2008). More recent surveillance data indicate that the prevalence of smoking and alcohol consumption remains substantial across Europe and in specific regional populations. According to the European Health Interview Survey, approximately 18.4% of adults in the European Union reported smoking cigarettes regularly, with prevalence rates varying between countries (Eurostat 2024). Similarly, data from the European Union drugs agency highlight that around 76.1% of young adults (15-34 years) in European countries have consumed alcohol at least once in the past year, with notable regional differences (EUDA 2025). These contemporary data underscore the relevance of lifestyle factors such as smoking and alcohol consumption in this population.
Alcohol and bone tissue
Alcohol consumption has complex effects on human bone tissue, with outcomes dependent on the level and pattern of consumption, frequency and personal characteristics. Heavy and chronic alcohol consumption is detrimental to bone health, primarily by suppressing osteoblast differentiation and activity, increasing oxidative stress within bone cells and disrupting endocrine signalling pathways critical for bone remodelling, such as alterations in parathyroid hormone, vitamin D metabolism and sex hormones (Chakkalakal 2006; Maurel et al. 2012). These mechanisms reduce bone formation, increase bone resorption and compromise bone strength, ultimately leading to osteopenia, osteoporosis and an increased risk of fractures. Additionally, alcohol consumption during critical periods of bone development, such as adolescence, can significantly hinder bone growth and development, resulting in decreased peak bone mass and density in both cortical and cancellous bones (Sampson et al. 1996). In adults, heavy alcohol use is known to induce secondary osteoporosis due to an imbalance in bone remodelling processes, characterised by suppressed bone formation and increased bone resorption (Mikosch 2014).
Conversely, light-to-moderate alcohol consumption may have a protective effect on bone health by modulating bone turnover markers, favouring increased osteocalcin and reduced resorption markers, which can help maintain bone mass, particularly in postmenopausal women and older adults. These beneficial effects are hypothesised to involve favourable hormonal balances and anti-inflammatory pathways. Importantly, the impact of alcohol on bone tissue strongly varies by dose, drinking pattern (e.g., binge versus regular moderate intake) and age and health status, underscoring the need for nuanced interpretation of observational findings (Gaddini et al. 2016). Overall, while moderate alcohol consumption may offer some benefits to bone health, particularly in specific populations, heavy and chronic alcohol consumption is a significant risk factor for bone-related diseases because of its multifaceted adverse effects on bone metabolism and structure (Broulík et al. 2010; Cho et al. 2018).
Smoking and bone tissue
Smoking has a significant and deleterious impact on human bone tissue, influencing bone health through various mechanisms. Tobacco smoke increases oxidative stress, inducing apoptosis of osteoblasts and impairing collagen synthesis, which results in a defective bone matrix and reduced bone quality (Al-Bashaireh et al. 2018). Smoking alters endocrine regulation by disrupting the parathyroid hormone-vitamin D axis and lowering circulating sex hormones, such as estrogen and testosterone, both of which are essential for maintaining a balance in bone remodelling. It also dysregulates the receptor activator of nuclear factor-kappa B ligand/osteoprotegerin (RANKL-RANK-OPG) pathway, increasing osteoclastogenesis and bone resorption (Al-Bashaireh et al. 2018). The effect of smoking on BMD has been well documented. Smokers generally exhibit reduced BMD compared to non-smokers, which translates to a higher risk of fractures, particularly in the hip and spine. This risk is dose-dependent and demonstrably higher in current smokers than in former smokers and non-smokers, emphasising the benefits of smoking cessation for bone health (Ward and Klesges 2001; Yoon et al. 2012). Cigarette smoking also exacerbates the risk of perioperative complications, such as nonunion, delayed union of fractures, infection and soft tissue complications. Brief preoperative smoking cessation can mitigate these risks to some extent, underscoring the importance of addressing smoking habits in medical and surgical settings (Lee et al. 2013). Despite the significant challenges posed by smoking on bone health, evidence in the literature suggests that the adverse effects of smoking are partly reversible. Smoking cessation can improve bone mass and reduce fracture risk, thereby offering a critical intervention strategy for mitigating the harmful effects of smoking on bone tissue (Al-Bashaireh et al. 2018; Yoon et al. 2012; Ward and Klesges 2001). These findings highlight the importance of incorporating smoking cessation strategies into public health efforts to improve bone health and prevent smoking-induced bone metabolic disorders (Weng et al. 2022).
Other lifestyle factors and bone tissue
In addition to smoking and alcohol, other lifestyle and physiological factors influence bone quality in young adults. Elevated blood pressure has been associated with altered bone remodelling and increased risk of bone fragility through mechanisms involving vascular and metabolic dysfunction (Hennen et al. 2025). Body composition parameters, notably fat mass and muscle mass, correlate with bone mineral density and structural bone integrity, reflecting the interaction of adiposity, muscle function and skeletal health (Geraldi et al. 2025; Tajaldeen et al. 2022). Physical activity is a critical modulator of bone mass acquisition and maintenance, enhancing bone strength via mechanical loading and biochemical signalling during early adulthood (Zhang et al. 2024). Moreover, despite extensive research on bone health in older adults, early adulthood remains notably underexplored, representing a critical gap in the literature. This age range, including typical university years, is crucial for achieving peak bone mass, which substantially influences lifelong skeletal health and fracture risk (Baxter-Jones et al. 2011; Dei and Succu 2024). In addition, university populations provide a unique setting to study lifestyle factors such as smoking and alcohol consumption, which often begin or intensify during this transitional phase, potentially impacting bone mass acquisition.
Therefore, the primary research question of this study is to investigate whether smoking and alcohol consumption, considering both quantity and duration, are associated with bone quality, as measured by radial quantitative ultrasound (QUS) Z-scores, in young adults. We hypothesise that higher smoking and alcohol use will be negatively associated with QUS Z-scores after adjusting for body composition and physical activity. This study aims to elucidate the complex relationships among these lifestyle factors and bone health during early adulthood, an understudied and critical period for peak bone mass acquisition.
Sample and methods
Sample
A sample of 1001 young Slovaks (303 men, 698 women), all aged 18 to 30 (22±2.35) years, was studied. The participants were primarily university students recruited through a non-random volunteer and convenience sampling procedure at the laboratory of the Department of Anthropology at Comenius University in Bratislava. The Ethics Committee of Comenius University Bratislava (protocol number ECH19021) approved the sample collection and analyses. Written informed consent was obtained from all participants in accordance with the Declaration of Helsinki, as amended in October 2013, after they were informed about the procedures used in the experiments. The only exclusion criterion applied was age; no other inclusion or exclusion criteria were applied.
Anthropometric analysis and blood pressure measurement
Trained anthropologists collected anthropometric data using internationally recognised methods (Lohman et al. 1988). Height was measured precisely to the nearest 0.5cm using a Siber and Hegner anthropometer. The InBody 770's integrated weight scale accurately recorded body weight with a precision of 0.1kg. A tape measure (Seca, Hamburg, Germany) was used to record their hip and waist measurements. To determine the body mass index (BMI), the weight in kilograms was divided by the square of the height in meters. The waist-to-hip ratio (WHR) was calculated by dividing the waist circumference by the hip circumference; for women, a ratio below 0.84 and for men, below 0.89, is deemed ideal (WHO 2000). The waist-to-height ratio (WHtR) was calculated by dividing the waist circumference by the subject's height; a ratio below 0.5 is generally considered ideal for both men and women, indicating reduced cardiometabolic risk (Gibson and Ashwell 2020). Blood pressure and heart rate were assessed in triplicate using a digital sphygmomanometer (Omron M3) and average values were used for analysis.
Body composition analysis
Body composition, specifically per cent body fat (PBF) and Skeletal muscle mass in kilograms (SMM), was assessed using the InBody 770 analyser (Biospace Co., Republic of Korea), which employs segmental multifrequency bioelectrical impedance analysis. To ensure precise results, measurements were taken under controlled conditions: participants refrained from physical activity for eight hours prior, avoided significant water and food intake for three hours before the test.
Bone quality measurement
QUS measurements were performed using the Sunlight MiniOmni device at the distal radius, with three to five repeated measurements per participant and daily calibration of the device. The measurement was taken at the midpoint between the olecranon process of the ulna and the tip of the distal phalanx of the middle finger, using ultrasound gel. The Z-score and speed of sound (SOS; m/s) were recorded, with higher readings indicating greater bone density. Although specific intra-session and inter-rater reliability statistics for our laboratory were not available, similar devices measuring at the radius have demonstrated good repeatability and inter-rater reliability, with intraclass correlation coefficient values close to 0.90 reported in the literature, supporting the precision and reliability of our measurements (Puranda et al. 2025).
Moreover, QUS and Dual-energy X-ray Absorptiometry (DXA) assess related but distinct properties of bone tissue. DXA directly measures BMD, while QUS evaluates parameters such as the SOS, which reflects both bone density and quality attributes. Multiple studies demonstrate moderate correlations between QUS and DXA measurements, supporting the convergent validity of QUS (Chanprasertpinyo et al. 2023; Natukunda et al. 2025; Swinton et al. 2023; Wang et al. 2008); however, differences in sensitivity and specificity indicate that QUS cannot replace DXA for the diagnosis of osteoporosis. Consequently, QUS (SOS/Z-score) values should not be interpreted as equivalent to DXA BMD and this distinction should be considered when interpreting our study findings.
Questionnaire
Alcohol consumption, smoking and physical activity data were collected using the WHO STEPS 2014 questionnaire (version 3.2), translated into Slovak and administered by trained personnel under standardised conditions (WHO 2014). In this study, the original WHO STEPS instrument, which has been validated and standardised internationally, was translated for use in the Slovak population. While a formal validation of the instrument in the Slovak context was not conducted, we implemented reliability checks within our sample, including assessments of internal consistency (Cronbach's alpha=0.73 and McDonald's omega=0.81).
The instrument covered medical history, diet and behaviours such as physical activity and alcohol consumption.
In this study, alcohol consumption was assessed using the aforementioned self-reported WHO questionnaire, measuring the average number of standard alcoholic beverages consumed per week. This measure captures habitual alcohol consumption behaviour, providing a helpful estimate of chronic exposure. Additionally, we calculated the estimated peak blood alcohol concentration using the Widmark formula, which takes into account the dose, body weight and distribution volume. Cmax reflects the highest concentration of ethanol in the bloodstream after a drinking episode and is biologically informative in bone research, as acute peak alcohol exposure can influence bone cells differently than average consumption levels. While the WHO questionnaire reflects consumption frequency and volume, Cmax provides insight into acute exposure and potential toxicity. This dual quantification approach allows for a comprehensive analysis of both habitual and peak alcohol effects on bone tissue. Although Cmax was not the primary analytic exposure, sensitivity analyses that included Cmax supported the robustness of the results.
The duration of alcohol consumption was obtained by including current alcohol consumers, thus, calculated by subtracting the answer to the question "How old are you?" from the answer to the question "How old were you when you started drinking alcohol?" and including past alcohol consumers by subtracting the age at which they started consuming alcohol from the age at which they stopped drinking. The second variable evaluated alcohol consumption based on the number of drinks consumed per week.
Similarly, smoking duration was evaluated by including current smokers by subtracting the number of years of smoking from the answer to the question "How old are you?" from the question "How old were you when you started smoking?", and past smokers by subtracting the age at which they started smoking from the age at which they stopped smoking. The second variable evaluated the smoking quantity, measured as the number of cigarettes per week.
Physical activity (PA) was evaluated by the minutes of PA per day, as analysed by the question "How much time do you spend on average doing sports per day?"
Statistics
A p-value threshold of p is less than 0.05 was used to determine the statistical significance. The data were analysed using jamovi (version 2.7.3) and R (4.4.1, package St. Nicolas House Analysis, SNHA). Descriptive statistics, including the student's t-test and Mann-Whitney U test, were used based on the data distribution assessed using the Kolmogorov-Smirnov test. Moreover, to account for the risk of false positives due to multiple comparisons, we applied the Benjamini-Hochberg procedure to adjust p-values in descriptive analyses; p-values were ranked in ascending order and the adjusted value for each test was calculated as p×N/rank, where N is the total number of tests and rank is the position in the ordered list. For values exceeding 1, the adjusted p-value was set to 1, and monotonicity was ensured by step-up correction. This approach controls the false discovery rate (FDR), maintaining the expected proportion of false positives below a set threshold (Benjamini and Hochberg 1995). Forward linear regression analysis was used to analyse the predictors, including diastolic blood pressure (DBP), PBF, SMM, PA, sex, smoking and alcohol consumption, of Z-score QUS. St. Nicolas House Analysis (Groth et al. 2019) was used to visualise and detect the interactions among the variables under study. A directed acyclic graph (DAG) was constructed using DAGitty (Textor et al. 2016) to clarify the hypothesised causal relationships between smoking and alcohol use (both quantity and duration), body composition, physical activity, sex and bone quality (Z-score). The DAG informed variable selection for model adjustment and helped to illustrate potential mediator and confounder structures in the analyses.
Results
The baseline characteristics of the participants, divided first by sex and then into alcohol consumers (AC; n=894) and abstainers (n=107), are presented in the supplement (Table 2 and 3). It includes the bone parameter Z-score in men AC (-0.30±0.97), men abstainers (-0.27±0.69), women AC (-0.21±1.06) and women abstainers (-0.20±1.17). Moreover, it illustrates body composition parameters, such as SMM, PBF, blood pressure and heart rate. No statistically significant differences were observed between the two groups, regardless of sex, for any of the variables. The only statistically significant difference observed was in the smoking duration (yrs), where men (p equals 0.014) who smoked AC smoked for longer (1.49±2.87 years) than those who abstained from smoking (0.51±2.05 years). The same trend was also observed in women (p equals 0.001), with AC smokers having smoked longer (years: 1.01±2.31) than abstainers (years: 0.31±1.39).
Additionally, among the participants, men started consuming alcohol on average at the age of 16.26±1.64 yrs, with the youngest aged 12 yrs and the oldest 23 yrs. A similar trend was observed in women (16.37±1.50 yrs), with the youngest and oldest being 11 and 21 years old, respectively. Men drank alcohol for 6.25±2.84 years, while women drank for 5.30±2.83 years.
The baseline characteristics of young adults categorised first by sex and then into smokers (n=227) and non-smokers (n=774) is also presented in the supplement (Table 3 and 4). It includes bone parameters, such as the Z-scores for men smokers (-0.31±0.98), men non-smokers (-0.32±0.93), women smokers (-0.22±0.99) and women non-smokers (-0.20±1.09). Additionally, it covers body composition parameters, blood pressure and heart rate. Statistically significant differences were observed mainly in women; smokers had a higher BMI (p=0.032) and PBF (%; p equals 0.003) than non-smokers. Moreover, among women smokers, it appeared that they drank alcohol longer than non-smokers (yrs; 5.72±2.82 vs. 5.17±2.83; p equals 0.049). Lastly, in smokers, both men (p equals 0.006) and women (p is less than 0.001), a higher Cmax is observed compared to non-smokers.
While several statistically significant differences were identified between alcohol consumers and abstainers (Table 2, 3) and smokers and non-smokers (Table 4, 5), most of these differences are of minimal clinical significance. For instance, smoking duration in men differed significantly between alcohol consumers (1.49±2.87 years) and abstainers (0.51±2.05 years, p=0.014; effect size =−0.20), but both groups exhibit relatively short smoking histories, with mean differences of <1 year, insufficient to substantially modify bone metabolism. Similarly, among women smokers, PBF was significantly higher (28.49±7.37%) than in non-smokers (26.59±7.24%, p equals 0.003; effect size =−0.16), representing a difference of approximately 1.9 percentage points. This difference, while statistically reliable, falls below clinical thresholds for metabolic risk stratification and does not alter health recommendations. Blood pressure differences between groups were even more trivial (<2mmHg), well below the 10mmHg threshold considered clinically meaningful in hypertension guidelines. In summary, despite statistical significance in selected comparisons, baseline characteristics were similar between groups.
In addition, among the male participants, the average age of starting smoking was 17.03±2.70 years, with the youngest being 9 years and the oldest 27 years. A similar trend was observed in women (17.09±1.90), with the youngest being 12 years old and the oldest 24 years old. Men and women smoked for 5.79±3.87 and 5.92±4.72 years, respectively.
Table 1 presents the findings of the linear regression analysis, which accounted for 5.0% of the variance in the radial QUS Z-scores (cap R squared equals 0.050), indicating limited explanatory power. The overall model was statistically significant (F(9.448)=2.609, p equals 0.006). Among the predictors, the duration of alcohol consumption in years emerged as a significant positive predictor of bone mineral density, with a standardised beta coefficient of 0.172 (p is less than 0.001). While statistically significant (p is less than 0.001), the minimal effect size (beta equals 0.172, with a 95%CI of [0.03, 0.10] per year of alcohol consumption) suggests limited practical clinical relevance. This suggests that a longer history of alcohol consumption is associated with higher Z-scores and thus higher bone mineral density. Importantly, PA was included as a covariate in this model and did not show a statistically significant relationship with Z-scores (beta equals 0.007, p equals 0.893), suggesting that the positive alcohol-bone association was not mediated or substantially confounded by differences in PA levels. Conversely, the number of cigarettes smoked per week was negatively significantly associated with BMD (beta equals minus 0.113, p equals 0.042), aligning with a potential negative impact on bone health. Other variables, including physical activity, smoking duration and body composition parameters (SMM and PBF), did not show a statistically significant relationship with Z-scores QUS. While the associations observed between lifestyle factors (smoking and alcohol consumption) and bone quality were statistically significant, the relatively lowcap R squared underscores that many other biological, environmental and genetic factors contribute to bone health beyond the variables included in our model. Therefore, the interpretation of our findings emphasises the presence of statistically significant relationships rather than the magnitude of variance explained.
In addition, an assessment of potential non-linearity and synergistic effects between smoking and alcohol consumption was examined. Centred variables and corresponding quadratic terms, as well as their interaction, were included in the regression model. None of these terms reached statistical significance (all p is greater than 0.4), nor did the overall model (F-test p equals 0.78). These findings indicate that, in our sample, there is no evidence of non-linear or synergistic associations between smoking and alcohol consumption.
Table 1 Association of Z-score QUS with sex, blood pressure, body composition, physical activity, smoking and alcohol consumption in young Slovaks (303 men, 698 women, age 22±2.35)
Dependent variables
Predictors
VIF
Unstandardised B
Standardised ꞵ
95 % CI
p
cap R 2
Adjusted
cap R 2
Lower
Upper
Z-score QUS
Sex (Women—Men)
4.43
0.148
0.143
-0.27
0.56
0.485
0.050
0.031
DBP (mmHg)
1.07
-0.009
-0.070
-0.02
0.02
0.143
PBF (%)
1.61
0.002
0.019
-0.01
0.02
0.752
SMM (kg)
4.00
-0.001
-0.004
-0.03
0.03
0.962
PA (min/day)
1.30
0.001
0.007
-0.01
0.01
0.893
Alcohol duration (yrs)
1.12
0.064
0.172
0.03
0.10
<0.001*
Alcohol (drinks/week)
1.15
0.000
0.000
-0.02
0.02
0.997
Smoking duration (yrs)
1.50
0.029
0.068
-0.02
0.08
0.230
Smoking (cigarettes/week)
1.46
-0.005
-0.013
-0.01
-0.00
0.042*
* Indicates statistical significance atp is less than 0.05. Abbreviations: B, beta coefficient; p, value of statistical significance (linear regression analysis, forward method); VIF, Variance Inflation Factor; cap R squared, coefficient of determination; Z-score QUS, Z-score quantitative ultrasound; DBP, Diastolic blood pressure; PBF, Per cent body fat; SMM, Skeletal muscle mass; PA, Physical activity; yrs, years; min/day, minutes per day; CI, Confidence Interval
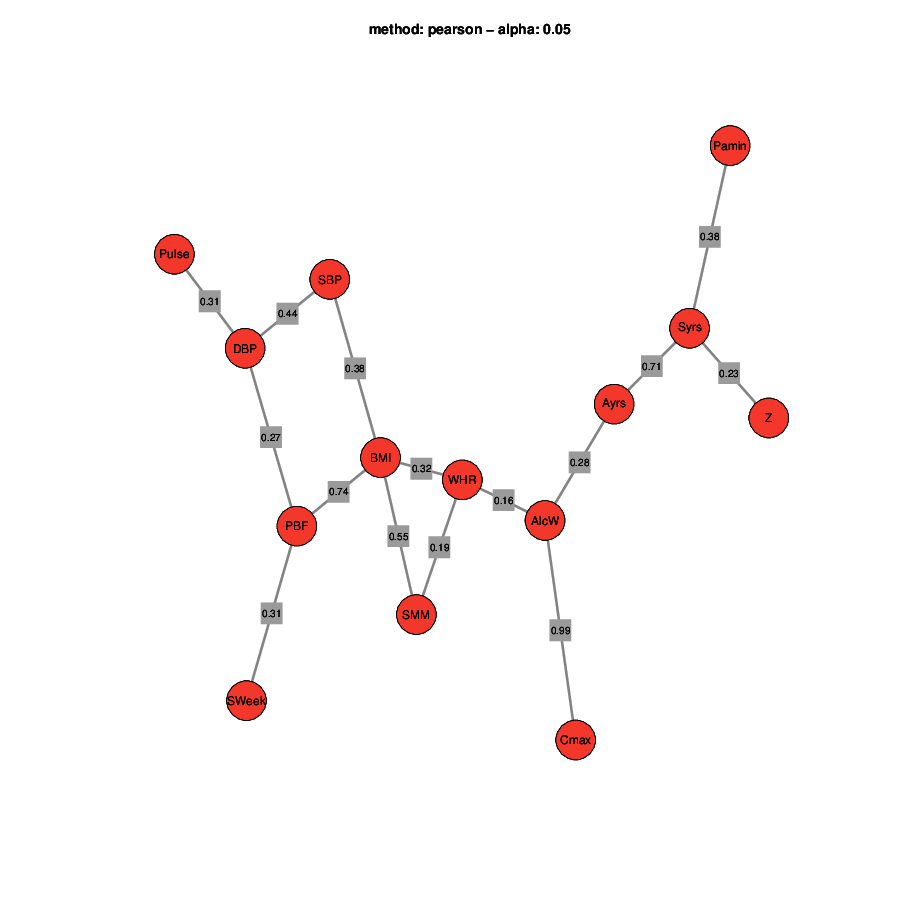
The SNHA with Pearson's correlation in men revealed several significant associations among the variables under study (Figure 1). A cluster of closely correlated variables grouped the body composition indices and blood pressure parameters. BMI was strongly positively correlated with PBF (r equals 0.74). Blood pressure parameters were found to be correlated with BMI and PBF. Alcohol consumption was strongly associated with blood alcohol concentration and weakly with WHR (r equals 0.16). Smoking behaviour showed a significant interaction with other lifestyle habits. The duration of smoking was strongly correlated with the duration of alcohol consumption (r equals 0.71), suggesting a co-occurrence of these two habits in the studied sample. A weaker correlation was observed between duration of smoking and the QUS Z-score (r equals 0.23), reflecting a potential association between smoking and skeletal health.
Figure 1 St. Nicholas House graph of variables influencing bone density concerning smoking and alcohol consumption of young Slovak men. Abbreviations: Pamin, physical activity (minutes/day); PBF, per cent body fat; SMM, Skeletal muscle mass (kg); BMI, Body mass index; WHR, waist-to-hip ratio; SBP, Systolic blood pressure (mmHg); DBP, diastolic blood pressure (mmHg); Z, Z-score QUS; Ayrs, duration of alcohol consumption (yrs); AlcW, number of alcoholic drinks consumed per week; Syrs, duration of smoking (yrs); Sweek, number of cigarettes smoked per week; Cmax, peak blood alcohol concentration. The numbers on the lines of the graph represent the Pearson correlation coefficients (r), which indicate the strength and direction of the association between variables.
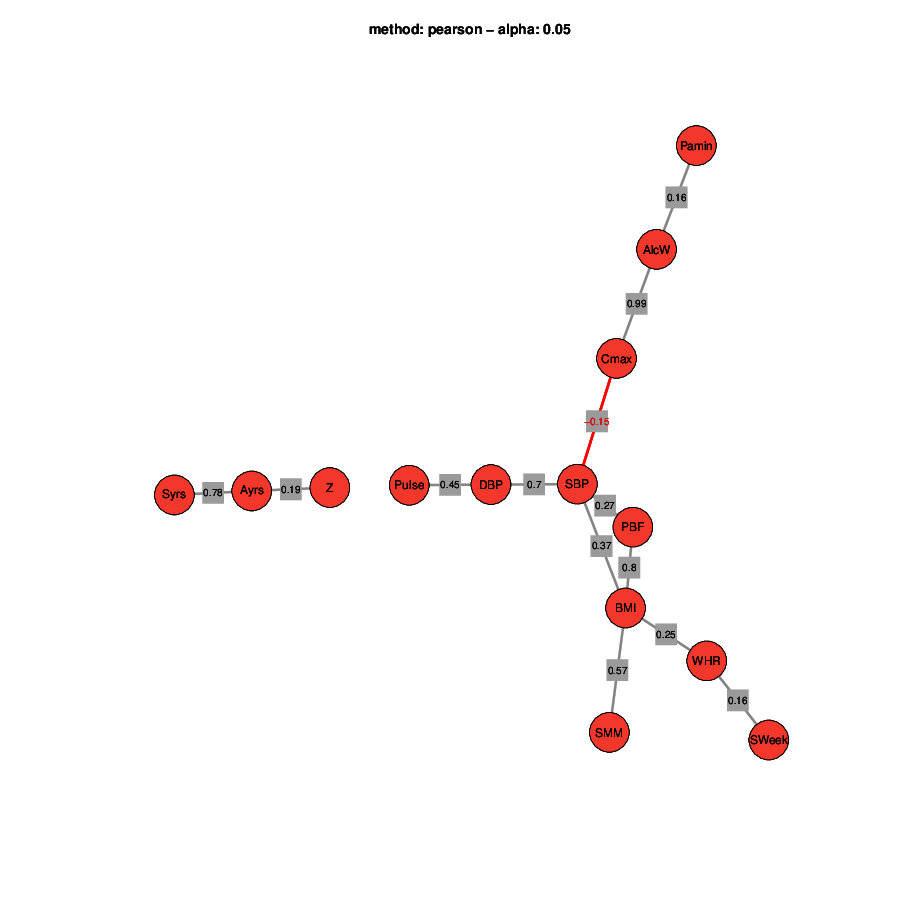
SNHA yielded similar results for women (Figure 2). Body composition variables and blood pressure parameters were closely associated. Specifically, BMI showed a strong positive correlation with PBF (r equals 0.80) and SBP showed a positive correlation with BMI of r equals 0.37. At the same time, Cmax was negatively correlated to SBP (r equals minus 0.15), indicating that alcohol consumption at higher concentrations is associated with lower SBP.
Smoking behaviour showed a significant interaction with other lifestyle factors. The duration of smoking was strongly correlated with the duration of alcohol consumption (r equals 0.78), suggesting similarly to the results found in men a co-occurrence of these two habits. A weaker correlation was observed between Ayrs and the QUS Z-score (r equals 0.19), indicating that those who drink longer have better bone quality and quantity.
Figure 2 St. Nicholas House graph of variables influencing bone density concerning smoking and alcohol consumption of young Slovak women. Abbreviations: Pamin, physical activity (minutes/day); PBF, per cent body fat; SMM, Skeletal muscle mass (kg); BMI, Body mass index; WHR, waist-to-hip ratio; SBP, Systolic blood pressure (mmHg); DBP, diastolic blood pressure (mmHg); Z, Z-score QUS; Ayrs, years of alcohol consumption; AlcW, number of alcoholic drinks consumed per week; Syrs, years of smoking; Sweek, number of cigarettes smoked per week; Cmax, peak blood alcohol concentration. The numbers on the lines of the graph represent the Pearson correlation coefficients (r), which indicate the strength and direction of the association between variables.
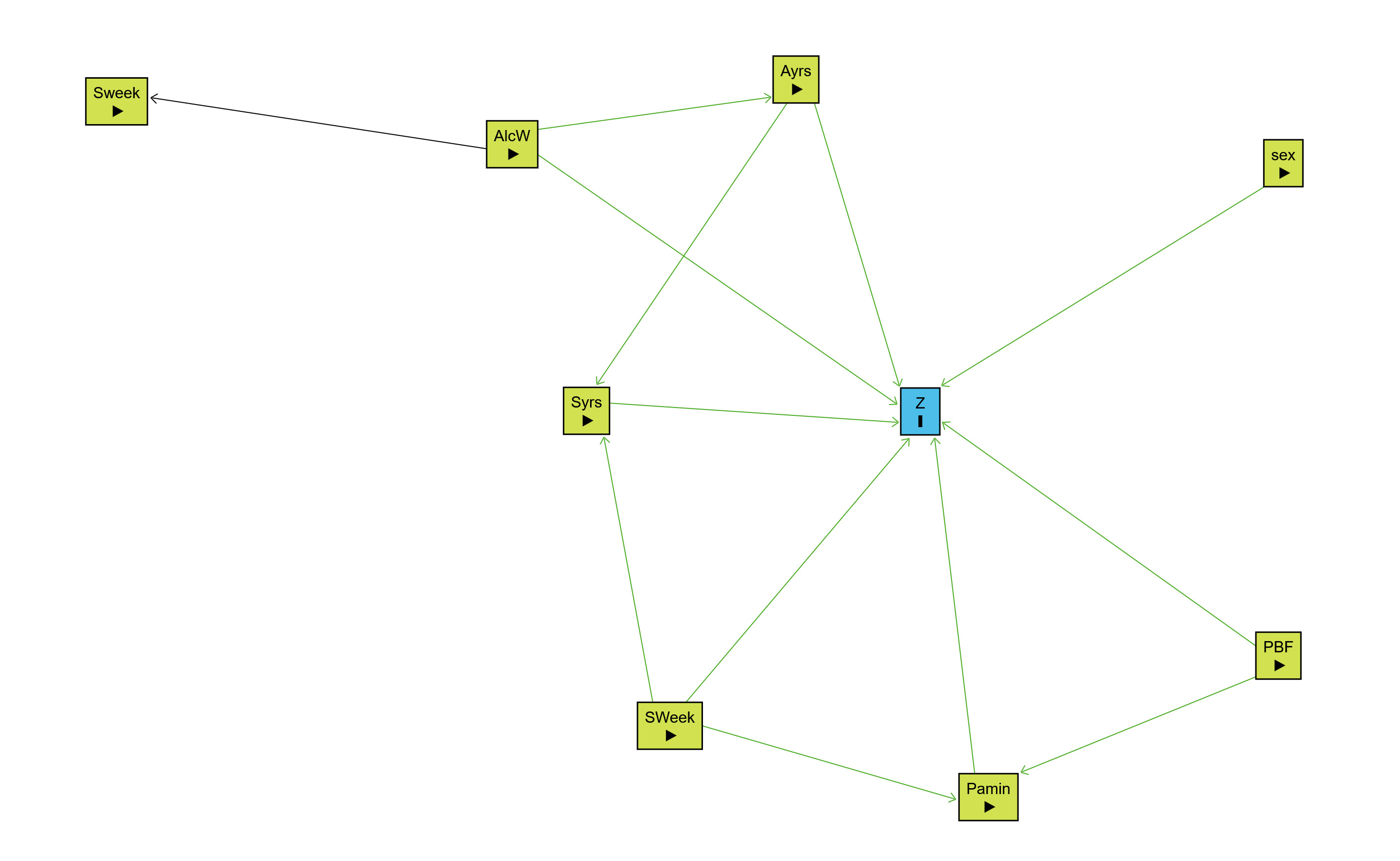
Figure 3 depicts the directed acyclic graph constructed to clarify the hypothesised causal relationships among the main variables under study. The DAG shows that both the quantity and duration of smoking, as well as the quantity and duration of alcohol consumption, are linked to Z-score both directly and indirectly via multiple pathways. Namely, alcohol quantity influences smoking behaviour, both in terms of amount and duration, illustrating their frequent co-occurrence in the sample. The model also highlights mediational relationships: smoking amount predicts smoking duration and alcohol quantity predicts alcohol duration, with both measures affecting bone quality. Physical activity and PBF are included as important covariates. PBF influences physical activity and has a direct effect on QUS Z-score, reflecting its recognised role in bone remodelling. Physical activity, in turn, affects QUS Z-score and is influenced by both PBF and smoking amount, representing behavioural and metabolic impacts on bone. Sex is also included with a direct path to Z-score, accounting for known physiological differences. Overall, the DAG clarifies how the constructs measured (quantity vs. duration) can yield different associations depending on the analytical approach, explaining the discrepancy between the results found in the regression analysis and network correlation findings (SNHA).
Figure 3 Directed acyclic graph of hypothesised causal relationships between smoking, alcohol, body composition, physical activity and bone quality (Z-score) of young Slovak men and women. Abbreviations: Pamin, physical activity (minutes/day); PBF, per cent body fat; Z, Z-score QUS; Ayrs, years of alcohol consumption; AlcW, number of alcoholic drinks consumed per week; Syrs, years of smoking; Sweek, number of cigarettes smoked per week; Cmax, peak blood alcohol concentration. Legend: Light green nodes, exposure variables; Blue node, primary outcome; arrows, hypothesised direction of causal relationship; each path, possible direct or mediated influence among the variables.
Discussion
The present study investigated the effects of alcohol consumption and smoking on bone health in a sample of young Slovak adults, an age group known for the high prevalence of these behaviours. The primary aim was to determine how bone quality (SOS-derived Z-score), measured using QUS, is related to smoking and alcohol consumption habits. This study is particularly relevant during the peak bone mass acquisition period, typically spanning the ages of 18 to 35, during which skeletal mass reaches its peak in life. In this phase, osteoblast-mediated bone formation typically exceeds bone resorption, resulting in positive bone balance. This physiological state is accompanied by optimal levels of sex hormones, particularly estrogen and testosterone, which regulate the balance between osteoblastic and osteoclastic activity (Bachrach 2001; Falahati-Nini et al. 2000; Soyka et al. 2000). Within this context, lifestyle factors such as smoking and moderate alcohol consumption are biologically plausible to have a less significant impact on bone tissue quality compared to their effect in older populations, where bone resorption surpasses formation and skeletal vulnerability to external insults increases (Taes et al. 2010; Yoon et al. 2012). This limited impact of lifestyle factors is further reinforced by the relatively short durations of smoking and alcohol exposure in young adults (typically a few years), which further reduces the likelihood of detectable deleterious effects on bone quality. This explains why our standardised effect sizes for smoking and alcohol are modest, aligning with the biological mechanisms and pathophysiology of the skeleton in this age range.
Alcohol and bone health
Alcohol consumption has significant effects on bone tissue, with the impact varying based on the level and pattern of alcohol intake. Chronic excessive alcohol consumption is associated with an increased risk for osteoporosis, characterised by an osteopenic skeleton and increased fracture risk. This is mainly due to decreased bone formation rather than increased bone resorption, as alcohol negatively affects osteoblast activity and suppresses the differentiation of bone marrow cells into osteoblasts, which are crucial for bone remodelling and formation (Chakkalakal 2006). However, our findings in this young adult population diverge substantially from this established literature. Contrary to the well-documented adverse effects of heavy and chronic alcohol use on bone mineral density (Broulík et al. 2010; Cho et al. 2018), our linear regression analysis revealed that the duration of alcohol consumption was a positive predictor of Z-score (beta equals 0.172, p is less than 0.001); the SNHA also confirmed these results in women. This result aligns with previous studies that have observed a protective or beneficial effect of light to moderate alcohol intake on bone health, particularly in specific populations, such as postmenopausal women (Gaddini et al. 2016; Godos et al. 2022). However, critical methodological considerations must accompany the interpretation of this finding. Our cross-sectional design prevents establishing causation, and the positive association is likely explained by substantial confounding rather than a true protective effect of alcohol. Specifically, several unmeasured or inadequately measured factors may explain the observed positive association through confounding mechanisms such as the nutritional status, since our study lacked a detailed dietary assessment. In the Slovak cultural context, moderate alcohol consumption typically occurs in food-accompanied, social dining settings rather than isolated alcohol consumption. Social drinkers likely have higher overall caloric and micronutrient intakes (calcium, vitamin D, protein), directly supporting bone health. Beyond nutritional patterns, social alcohol consumption habits in this population may also correlate with higher levels of physical activity and mechanical loading, another confounding factor that impacts bone health. Regarding PA as a potential confounder, we explicitly examined this possibility given the central role of mechanical loading in bone adaptation (Frost 1987). Notwithstanding the theoretical plausibility of PA as a pathway linking alcohol consumption to bone outcomes, our regression analysis showed that PA was not a significant predictor of QUS Z-scores (p equals 0.893) and did not materially alter the positive alcohol-bone association when included in the multivariable model. Furthermore, baseline characteristics revealed no significant differences in physical activity levels between alcohol consumers and abstainers (p is greater than 0.40 across both sexes). These findings suggest that PA does not explain the observed positive association between alcohol duration and bone quality in our sample. However, this does not exclude the possibility that other unmeasured activities impacting mechanical loading, such as occupational physical activity or sport-specific impacts, may contribute to the observed associations. These confounding mechanisms may operate differentially across sexes, as evidenced by the subtle sex-specific patterns we observed in the associations between lifestyle factors and bone quality. Although both men and women showed the protective effect of alcohol duration on radial QUS Z-scores, the correlation strength differed, suggesting that sex hormones may modulate the relationship between alcohol and skeletal metabolism. To explain these differential responses, it is noteworthy that in men, estrogen plays a dominant role in regulating bone resorption, while both estrogen and testosterone are important in maintaining bone formation. Specifically, estrogen predominantly acts on trabecular bone through estrogen receptors alpha and beta, suppressing osteoclast activity and bone resorption, whereas testosterone exerts its effects on cortical bone through androgen receptors, promoting periosteal apposition and bone strength (Falahati-Nini et al. 2000; Khosla et al. 2001). It is possible that in a young adult population with a relatively short history of alcohol consumption, the pattern of alcohol consumption is more aligned with light to moderate intake rather than chronic heavy use, which could explain the observed positive association. These results were confirmed by the SNHA, where a positive correlation (r=0.19) was observed in women between the duration of alcohol consumption and the Z-score QUS. However, this finding also highlights the complexity of alcohol's effects on bone tissue and underscores the need for more research into the specific type, quantity and pattern of alcohol consumption in this age group. The diversity in alcohol's impact, from potential benefits at low to moderate levels of consumption to detrimental effects with heavy alcohol consumption, suggests that further research is needed to delineate the dose-response impact and to develop guidelines that protect bone health while considering alcohol consumption, especially since there are no uniform international guidelines available. The unexpected positive association between alcohol duration and bone health in our young sample may be explained by distinct physiological mechanisms operating during early adulthood. During late adolescence and young adulthood (18-30 years), individuals are still approaching or have recently achieved peak bone mass. At this life stage, bone formation typically exceeds bone resorption. Thus, light-to-moderate alcohol consumption at this age may not yet induce the oestrogen-suppressive and calcium-malabsorptive effects characteristic of chronic heavy alcohol consumption in older populations (Bachrach 2001; Benton et al. 2022; Soyka et al. 2000; Sripanyakorn et al. 2009). Additionally, the positive association observed in our study may reflect a cohort effect, where individuals with longer alcohol consumption histories are more likely to have better social integration, greater physical activity, or improved nutritional status, all factors that support bone accretion during the peak bone mass acquisition phase (Tsao et al. 2024).
Cultural and dietary factors influencing bone health in the Slovak population
The Slovak Republic possesses distinctive dietary and lifestyle patterns that may influence the bone health outcomes observed in this study of young adults. Central European populations, including Slovaks, traditionally maintain moderate to high consumption of dairy products, which represent significant sources of dietary calcium and phosphorus essential for bone development during peak bone mass acquisition. The literature shows that Slovak consumers' spending on food and non-alcoholic beverages comprises approximately 23.1% of household expenditure, with recent decades showing increased consumption of dairy products, fruits and vegetables, indicating a gradual shift toward healthier dietary patterns (Kubicová and Kádeková 2016; Mertens et al. 2019; Stefler et al. 2016; Ivaničová et al. 2024) . However, vitamin D levels in the Slovak population remain low. A cross-sectional study of medication-free Slovak adults revealed that 41% of the population exhibited insufficient or deficient 25-hydroxyvitamin D levels (is less than or equal to 30ng/ml), with physical inactivity, elevated blood pressure and smoking status strongly associated with lower vitamin D concentrations (Sebekova et al. 2016). This finding aligns with broader Central European patterns, where vitamin D deficiency is highly prevalent across the region. The Czech Republic, with dietary patterns similar to those of Slovakia, demonstrated even higher deficiency rates among adolescents and young adults (6-30 years: 77.9% with vitamin D insufficiency), particularly during the winter and spring months (Holmannova et al. 2025). These seasonal variations in vitamin D status may significantly impact skeletal metabolism during the critical period of peak bone mass acquisition in young adulthood, particularly through effects on the RANKL-RANK-OPG signalling pathway and parathyroid hormone regulation (Lips et al. 2019; Mertens et al. 2019).
Regarding alcohol consumption patterns, Slovakia exhibits characteristics that are distinct from those of other European regions. The Central European alcohol consumption pattern typical of Slovakia is characterised primarily by beer consumption, with increasing trends in fruit spirits consumption in recent decades. This cultural context of moderate, habitual alcohol consumption may partially explain the positive association observed in our study between longer alcohol duration and better bone health outcomes in young adults, as this pattern likely reflects social integration and potentially superior nutritional status compared to abstinence (Popova et al. 2007). These population-specific factors, including traditional dairy-based dietary components, widespread vitamin D insufficiency, particularly during winter months and culturally distinct alcohol consumption patterns emphasising social context, should be considered when interpreting the results of this cross-sectional study and when generalising findings to other European or non-European populations.
Smoking and bone health
Cigarette smoking is a significant risk factor for reduced BMD and osteoporosis. It contributes to bone deterioration through various pathways, including hormonal and metabolic disruptions (Ratajczak et al. 2021). Moreover, smoking during young adulthood has notable implications for bone health, potentially impacting bone mass acquisition and increasing the risk of osteoporosis later in life (Taes et al. 2010). Our analysis confirmed our hypothesis regarding the negative impact of smoking on bone health. The number of cigarettes smoked per week was identified as a significant negative predictor of Z-score (beta equals minus 0.113, p equals 0.042). This result is consistent with a large body of literature that demonstrates the harmful effects of tobacco smoking on BMD and fracture risk by altering calcium absorption, sex hormone regulation and increasing oxidative stress (Al-Bashaireh et al. 2018; Ward and Klesges 2001; Yoon et al. 2012). At the cellular level, smoking effects were consistent across sexes in our study, reflecting the universally detrimental impact of tobacco exposure through the RANKL-RANK-OPG pathway dysregulation. Tobacco smoke compounds, including cadmium and other toxins, directly impair osteoblast differentiation and promote osteoclast activation through the RANKL-RANK-OPG pathway, exacerbating bone resorption. RANKL, expressed by osteoblasts, binds to RANK receptors on osteoclast precursors, promoting their differentiation and activation. In contrast, OPG acts as a decoy receptor, inhibiting this process. Smoking exposure increases the RANKL/OPG ratio, thereby promoting enhanced osteoclast activity and bone resorption (Al-Bashaireh et al. 2018; Shahbaz et al. 2025; Xie et al. 2024). In younger populations, these structural impairments are important, as smoking during the peak bone mass acquisition phase compromises the establishment of optimal skeletal strength, with a long-term increase in fracture risk. However, the relationship between smoking intensity and bone tissue is more nuanced than this straightforward dose-response pattern might suggest. The SNHA exhibited contrasting results, showing elevated Z-score QUS values among individuals with a prolonged smoking duration (r=0.23). This discrepancy, where regression analysis identified smoking quantity as a negative predictor while the SNHA revealed weak positive correlations with smoking duration, reflects the complex associations between cumulative exposure (duration) and current smoking intensity (cigarettes/week). The DAG clarifies this distinction: smoking amount may predict both duration and quantity, but their independent effects on bone differ. Individuals with longer smoking histories may have established compensatory metabolic adjustments or may represent a cohort with inherently more resilient bone structure. Furthermore, the chronic and long-term effects of smoking on bone tissue may not be fully evident in a younger population, potentially leading to the observed association with improved bone health, which could be misleading. In addition, in this analysis, the correlations between bone tissue and smoking in both men and women were weak and likely influenced by the stronger association with the duration of alcohol consumption.
While the regression analysis identified alcohol duration and smoking quantity as statistically significant predictors of QUS Z-scores, the extremely low coefficient of determination (cap R squared equals 0.050) demands careful interpretation: these lifestyle factors account for only 5.0% of the variance in bone tissue quality in our sample of young adults, indicating they are minor contributors to skeletal outcomes. This limited explanatory power reflects the inherent multifactorial nature of bone health during the acquisition of peak bone mass. Unmeasured determinants, such as genetic predisposition, nutritional biomarkers (including vitamin D and calcium availability), hormonal profiles (including sex hormones, parathyroid hormones and growth factors), bone turnover markers and biomechanical loading, likely account for the majority of skeletal variation. Notably, despite statistical significance, the narrow confidence intervals for both predictors (alcohol duration: 95%CI [0.03,0.10]; smoking quantity: 95%CI [−0.01,−0.00]) underscore the minimal practical effect sizes, particularly for smoking. Although statistically significant, smoking and alcohol consumption show limited clinical relevance in this young population compared to other skeletal determinants.
Public Health Implications and Prevention Strategies
Given the high prevalence of smoking and alcohol consumption among young adults, our findings highlight several important public health implications. Integrating bone health assessments into routine health screenings for young adults, particularly within university populations, could facilitate the early identification of individuals at risk (Guglielmi and Terlizzi 2009; Nicholson et al. 2025). Since smoking exerts a dose-dependent adverse impact on bone quality, cessation of smoking can facilitate a partial restoration of bone density, thereby diminishing the risk of fractures later in life (Al-Bashaireh et al. 2018; Yoon et al. 2012). Therefore, public health initiatives should prioritise smoking cessation interventions for young adults. Despite the observed positive associations with light-to-moderate alcohol intake, public messaging must stress that alcohol is not recommended for bone health benefits, given its known risks at high consumption levels and among vulnerable populations. In conclusion, addressing broader determinants, such as nutrition, physical activity and maintaining a healthy body composition, is crucial for the effective prevention of future bone conditions. Ongoing research and the formulation of age-specific guidelines to promote bone health in young adults are essential.
Limitations
The cross-sectional design prevents the establishment of causality; future studies are necessary to determine the temporal relationships between smoking, alcohol consumption and bone health. Additionally, the sample consisted primarily of university students recruited through convenience sampling, which limits the generalizability of the findings to the broader young adult population in Slovakia. University students systematically differ in socioeconomic status, health behaviours and lifestyle clustering compared to non-university peers, potentially explaining the modest effect sizes observed in our analyses. Future research should employ representative, population-based sampling across diverse socioeconomic strata. The self-reported nature of the questionnaire data on smoking, alcohol consumption and physical activity introduces the possibility of reporting bias, which could influence the accuracy of our results. Another limitation is that we did not investigate other smoking types, such as vaping, but only cigarette smoking. Finally, several unmeasured variables likely influence bone outcomes, including nutritional biomarkers (such as vitamin D and calcium), hormonal profiles (including sex hormones and parathyroid hormones), bone turnover markers and mechanical loading. Moreover, although PA was included as a covariate in our regression model, a fundamental limitation is the reliance on self-reported PA as a sole indicator for mechanical loading, which may not comprehensively represent the full spectrum of mechanical loading. Occupational PA, habitual movement patterns and sport-specific impacts, are not adequately captured by this assessment. As a result, it is not possible to rule out the possibility of residual confounding due to aspects of PA that are either unmeasured or not measured adequately, and future studies should employ more comprehensive assessments of mechanical loading using objective measurements. Future research should address these limitations and expand the sample to include a more diverse population.
Conclusion
The present study revealed the contrasting effects of smoking and alcohol consumption on bone health in young Slovak adults. We found that smoking had an adverse impact, with the number of cigarettes smoked per week being a significant predictor of lower bone mineral density. This finding is consistent with the established literature and underscores the need for public health initiatives to promote smoking cessation. Conversely, our analysis showed an unexpected positive association between the duration of alcohol consumption and bone tissue quality. This result may be due to the prevalence of light-to-moderate alcohol consumption in this young population, which aligns with previous research suggesting a beneficial effect of moderate alcohol intake.
Authors contribution
Simona Sulis contributed to writing the manuscript, conceptualising it, collecting data and performing the statistical analysis. Lenka Vorobeľová and Darina Falbová designed the study, participated in data collection, reviewed and edited the manuscript. Alexandra Hozáková participated in the data collection and writing of the manuscript. All authors have read and agreed to the published version of this manuscript.
Appendix
Supplementary Tables
Table 2 Baseline body composition and bone quality characteristics of alcohol consumers and teetotallers of Slovak young women (n=698, 18-30 years)
Alcohol consumers (n=623)
Abstainers (n=75)
95% CI
Mean
SD
Mean
SD
Effect size
Upper
Lower
p
p FDR
Age
21.31
2.29
21.62
2.15
-0.02
-0.18
0.30
0.811 b
0.936
Height (cm)
166.73
6.07
165.98
6.28
0.12
-0.12
0.37
0.321a
0.803
Body mass (kg)
60.90
10.89
59.89
12.29
-0.11
-0.16
0.33
0.134b
0.670
BMI
21.84
3.59
21.68
4.00
-0.08
-0.20
0.29
0.264b
0.990
WHR
0.74
0.06
0.74
0.06
-0.08
-0.14
0.35
0.285b
0.855
WHtR
0.42
0.05
0.41
0.05
0.01
-0.23
0.26
0.908a
0.973
PBF (%)
26.94
7.31
27.44
7.25
0.03
-0.31
0.18
0.669b
1.000
SMM (kg)
23.89
3.09
23.17
3.20
0.23
-0.01
0.47
0.061a
0.458
DBP (mmHg)
69.61
8.00
70.41
9.33
0.03
-0.34
0.15
0.707 b
1.000
SBP (mmHg)
117.29
11.11
116.86
11.20
-0.02
-0.21
0.28
0.795b
0.994
Pulse (bpm)
79.74
12.90
81.16
12.77
-0.11
-0.35
0.13
0.376a
0.806
SOS (m/s)
4076.13
115.51
4081.15
114.36
-0.04
-0.29
0.20
0.725a
0989
Z-score QUS
-0.21
1.06
-0.20
1.17
-0.00
-0.25
0.24
0.977a
0.977
Smoking duration (yrs)
1.01
2.31
0.31
1.39
-0.16
0.07
0.56
0.001*b
0.015*
Physical activity (min/day)
66.99
41.90
69.00
59.44
0.05
-0.44
0.05
0.405b
0.759
* p is less than 0.05; a student t test; b Mann-Whitney U; CI, confidence interval; FDR, False Discovery Rate; BMI, Body mass index; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio; PBF, percent body fat; SMM, skeletal muscle mass; DBP, diastolic blood pressure; SBP, systolic blood pressure; SOS, speed of sound; QUS, Quantitative Ultrasound; yrs, years; min/day, minutes per day
Table 3 Baseline body composition and bone quality characteristics of alcohol consumers and teetotallers of Slovak young men (n=303,18-30 years)
Alcohol consumers (n=271)
Abstainers (n=32)
95% CI
Mean
SD
Mean
SD
Effect size
Upper
Lower
p
p FDR
Age
22.63
2.45
22.22
2.19
0.09
-0.11
0.29
0.366a
0.784
Height (cm)
180.58
7.25
181.89
7.45
0.01
-0.19
0.21
0.334a
0.835
Body mass (kg)
77.92
13.60
79.90
16.81
-0.00
-0.20
0.20
0.450a
0.844
BMI
23.85
3.58
24.04
4.26
-0.03
-0.42
0.31
0.791b
0.989
WHR
0.81
0.05
0.80
0.06
0.08
-0.13
0.28
0.761a
1.268
WHtR
0.45
0.05
0.45
0.05
0.01
-0.35
0.38
0.941a
0.941
PBF (%)
17.10
7.07
18.48
7.46
0.12
-0.56
0.17
0.255b
0.956
SMM (kg)
36.44
5.36
36.24
5.86
0.08
-0.13
0.28
0.849a
0.910
DBP (mmHg)
70.65
8.64
72.87
8.69
-0.15
-0.35
0.06
0.177a
1.00
SBP (mmHg)
133.27
12.51
130.09
16.46
0.09
-0.11
0.30
0.196a
0.980
Pulse (bpm)
75.51
13.49
78.03
12.24
-0.13
-0.34
0.07
0.321a
0.963
SOS (m/s)
4024.13
118.13
4028.47
84.73
-0.04
-0.24
0.16
0.840a
0.450
Z-score QUS
-0.30
0.97
-0.27
0.69
-0.02
-0.22
0.18
0.764a
1.00
Smoking duration (yrs)
1.49
2.87
0.51
2.05
-0.20
-0.02
0.72
0.014*b
0.210
Physical activity (min/day)
92.03
94.39
97.71
74.70
-0.02
-0.23
0.18
0.775a
1.00
*p is less than 0.05; a student t test; b Mann-Whitney U; CI, confidence interval; FDR, False Discovery Rate; BMI, Body mass index; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio; PBF, percent body fat; SMM, skeletal muscle mass; DBP, diastolic blood pressure; SBP, systolic blood pressure; SOS, speed of sound; QUS, Quantitative Ultrasound; yrs, years; min/day, minutes per day
Table 4 Baseline body composition and bone quality characteristics of smokers and non-smokers of Slovak young women (n=698, 18-30 years)
Smokers (n=149)
Non-smokers (n=549)
95% CI
Mean
SD
Mean
SD
Effect size
Upper
Lower
p
p FDR
Age
21.76
2.32
21.74
2.27
-0.01
-0.17
0.19
0.908 b
1.000
Height (cm)
166.69
6.14
166.69
6.09
-0.03
-0.21
0.15
0.764a
1.000
Body mass (kg)
61.99
11.76
60.36
10.82
-0.09
-0.03
0.33
0.109b
0.250
BMI
22.30
3.67
21.70
3.61
-0.11
-0.02
0.35
0.032*b
0.128
WHR
0.75
0.07
0.74
0.06
-0.10
0.02
0.38
0.062b
0.165
WHtR
0.43
0.05
0.42
0.05
0.24
0.06
0.43
0.009*a
0.048*
PBF (%)
28.49
7.37
26.59
7.24
-0.16
0.08
0.44
0.003b *
0.024*
SMM (kg)
23.89
3.29
23.79
3.06
0.03
-0.15
0.21
0.728 a
1.000
DBP (mmHg)
70.09
7.74
69.59
8.25
-0.04
-0.12
0.24
0.492b
0.875
SBP (mmHg)
117.45
7.74
117.18
11.09
-0.01
-0.16
0.21
0.808b
1.000
Pulse (bpm)
79.83
12.71
79.90
12.94
-0.01
-0.19
0.18
0.951a
0.951
SOS (m/s)
4077.36
99.58
4076.46
119.31
0.01
-0.17
0.19
0.933 a
0.995
Z-score QUS
-0.22
0.99
-0.20
1.09
-0.01
-0.19
0.17
0.914 a
1.000
Alcohol duration (yrs)
5.72
2.82
5.17
2.83
0.19
0.00
0.39
0.049*a
0.157
Cmax (%)
2.08
1.62
1.21
1.36
0.61
0.38
0.84
<0.001*a
0.016*
Physical activity (min/day)
62.64
34.92
68.25
45.60
-0.28
-0.46
-0.10
0.227a
0.454
*p is less than 0.05; a student t test; b Mann-Whitney U; CI, confidence interval; FDR, False Discovery Rate; BMI, Body mass index; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio; PBF, percent body fat; SMM, skeletal muscle mass; DBP, diastolic blood pressure; SBP, systolic blood pressure; SOS, speed of sound; QUS, Quantitative Ultrasound; Cmax, peak blood alcohol concentration; yrs, years; min/day, minutes per day
Table 5 Baseline body composition and bone quality characteristics of smokers and non-smokers of Slovak young men (n=303, 18-30 years)
Smokers (n=78)
Non-smokers (n=225)
95% CI
Mean
SD
Mean
SD
Effect size
Upper
Lower
p
p FDR
Age
22.65
2.60
22.57
2.36
0.04
-0.22
0.29
0.784a
1.000
Height (cm)
180.53
6.78
180.78
7.44
-0.03
-0.29
0.22
0.798 a
1.000
Body mass (kg)
77.64
11.70
78.30
14.68
-0.05
-0.30
0.21
0.722 a
1.000
BMI
23.81
3.21
23.89
3.80
-0.02
-0.28
0.23
0.863a
1.000
WHR
0.81
0.04
0.80
0.05
0.19
-0.07
0.45
0.148a
0.592
WHtR
0.45
0.04
0.45
0.05
0.09
-0.17
0.35
0.501a
1.000
PBF (%)
17.46
6.74
17.17
7.25
-0.04
-0.22
0.30
0.614b
1.000
SMM (kg)
36.13
4.86
36.52
5.58
-0.07
-0.33
0.19
0.585a
1.000
DBP (mmHg)
71.14
4.86
70.79
8.32
0.04
-0.22
0.30
0.766a
1.000
SBP (mmHg)
130.94
12.18
133.63
13.20
-0.21
-0.47
0.05
0.116a
0.619
Pulse (bpm)
75.38
12.55
75.91
13.66
-0.04
-0.30
0.22
0.966a
0.966
SOS (m/s)
4025.44
124.85
4024.30
111.61
0.01
-0.25
0.27
0.940a
1.000
Z-score QUS
-0.31
0.98
-0.32
0.93
0.01
-0.25
0.27
0.954a
1.000
Alcohol duration (yrs)
6.72
2.92
6.06
2.79
0.23
-0.05
0.51
0.105a
0.840
Cmax (%)
2.30
2.18
1.48
1.85
0.42
0.12
0.72
0.006*a
0.096
Physical activity (min/day)
91.88
76.49
92.75
97.39
-0.02
0.28
0.24
0.948a
1.000
*p is less than 0.05; a student t test; b Mann-Whitney U; CI, confidence interval; FDR, False Discovery Rate; BMI, Body mass index; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio; PBF, percent body fat; SMM, skeletal muscle mass; DBP, diastolic blood pressure; SBP, systolic blood pressure; SOS, speed of sound; QUS, Quantitative Ultrasound; Cmax, peak blood alcohol concentration; yrs, years; min/day, minutes per day
Acknowledgements
We thank the Department of Anthropology of the Faculty of Natural Sciences of Comenius University in Bratislava, Slovakia, and the participants whose involvement in this study made this study possible. We also thank Prof. Dr. Christiane Scheffler, Prof. Dr. Michael Hermanussen and Dr. Detlef Groth for their guidance in the analysis and conceptualisation process of the manuscript during the 8th Summer School "Human Growth and Development – Data Analysis and Statistics" in Gülpe, Germany, 2025, funded by KoUP. The study was financed by The Ministry of Education, Science, Research and Sport of the Slovak Republic, Grant/Award Number: KEGA 046UK-4/2023 and by Comenius University Bratislava (Grant number: UK/1007/2025; Grant project title: Energy drinks and eating habits impact on peripheral skeletal quality and health in early adulthood). Participation in the summer school was funded by the Erasmus+ programme.
References
Al-Bashaireh, A. M./Haddad, L. G./Weaver, M./Chengguo, X./Kelly, D. L./Yoon, S. (2018). The Effect of Tobacco Smoking on Bone Mass: An Overview of Pathophysiologic Mechanisms. Journal of Osteoporosis 2018 (1), 1–17. https://doi.org/10.1155/2018/1206235.
Baxter-Jones, A. D. G./Faulkner, R. A./Forwood, M. R./Mirwald, R. L./Bailey, D. A. (2011). Bone mineral accrual from 8 to 30 years of age: An estimation of peak bone mass. Journal of Bone and Mineral Research 26 (8), 1729–1739. https://doi.org/10.1002/jbmr.412.
Benjamini, Y./Hochberg, Y. (1995). Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. Journal of the Royal Statistical Society 57 (1), 289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x.
Benton, M. L./Jimenez, V. A./Newman, N./Gonzales, S. W./Grant, K. A./Turner, R. T./Iwaniec, U. T./Baker, E. J. (2022). Dose-response effects of alcohol on biochemical markers of bone turnover in non-human primates: Effects of species, sex and age of onset of drinking. Bone Reports 16, 101159. https://doi.org/10.1016/j.bonr.2021.101159.
Broulík, P. D./Vondrová, J./Růžička, P./Sedláček, R./Zíma, T. (2010). The Effect of Chronic Alcohol Administration on Bone Mineral Content and Bone Strength in Male Rats. Physiol Research, 599–604. https://doi.org/10.33549/physiolres.931799.
Burg, R. von (1982). E. M. P. Widmark, Principles and applications of medicolegal alcohol determination translated from the original publication in 1932 by R. C. Baselt. Biomedical Publications, Davis California, 166 pp., $53.00. Journal of Applied Toxicology 2 (5), IV. https://doi.org/10.1002/jat.2550020515.
Chanprasertpinyo, W./Punsawad, C./Khwanchuea, R./Sukkriang, N./Yincharoen, P./Rerkswattavorn, C. (2023). Comparison between calcaneus quantitative ultrasound and the gold standard DXA in the ability to detect osteoporosis in chronic obstructive pulmonary disease patients. Journal of Orthopaedic Surgery and Research 18 (1), 778. https://doi.org/10.1186/s13018-023-04211-8.
Cho, Y./Choi, S./Kim, K./Lee, G./Park, S. M. (2018). Association between alcohol consumption and bone mineral density in elderly Korean men and women. Archives of Osteoporosis 13 (1), 46. https://doi.org/10.1007/s11657-018-0462-4.
Dei, M./Succu, C. (2024). Bone fragility in young people: significant anamnestic elements. International Journal of Bone Fragility 4 (1), 11–15. https://doi.org/10.57582/IJBF.240401.011.
EUDA (2025). Statistical Bulletin 2025.
Eurostat (2024). European Health Interview Survey 2024.
Falahati-Nini, A./Riggs, B. L./Atkinson, E. J./O'Fallon, W. M./Eastell, R./Khosla, S. (2000). Relative contributions of testosterone and estrogen in regulating bone resorption and formation in normal elderly men. The Journal of Clinical Investigation 106 (12), 1553–1560. https://doi.org/10.1172/JCI10942.
Gaddini, G. W./Turner, R. T./Grant, K. A./Iwaniec, U. T. (2016). Alcohol: A Simple Nutrient with Complex Actions on Bone in the Adult Skeleton. Alcoholism: Clinical and Experimental Research 40 (4), 657–671. https://doi.org/10.1111/acer.13000.
Geraldi, M. V./Gregori, G./Johansson, L./Hjertonsson, U./Brättemark, E./Lorentzon, M. (2025). Associations between body composition and bone loss in early postmenopausal women. Journal of Bone and Mineral Research (zjaf125), 1–8. https://doi.org/10.1093/jbmr/zjaf125.
Gibson, S./Ashwell, M. (2020). A simple cut-off for waist-to-height ratio (0·5) can act as an indicator for cardiometabolic risk: recent data from adults in the Health Survey for England. The British Journal of Nutrition 123 (6), 681–690. https://doi.org/10.1017/S0007114519003301.
Godos, J./Giampieri, F./Chisari, E./Micek, A./Paladino, N./Forbes-Hernández, T. Y./Quiles, J. L./Battino, M./La Vignera, S./Musumeci, G./Grosso, G. (2022). Alcohol Consumption, Bone Mineral Density, and Risk of Osteoporotic Fractures: A Dose–Response Meta-Analysis. International Journal of Environmental Research and Public Health 19 (3), 1515. https://doi.org/10.3390/ijerph19031515.
Groth, D./Scheffler, C./Hermanussen, M. (2019). Body height in stunted Indonesian children depends directly on parental education and not via a nutrition mediated pathway - Evidence from tracing association chains by St. Nicolas House Analysis. Anthropologischer Anzeiger; Bericht uber die biologisch-anthropologische Literatur 76 (5), 445–451. https://doi.org/10.1127/anthranz/2019/1027.
Harrison, E. L. R./Desai, R. A./McKee, S. A. (2008). Nondaily smoking and alcohol use, hazardous drinking, and alcohol diagnoses among young adults: findings from the NESARC. Alcoholism: Clinical and Experimental Research 32 (12), 2081–2087. https://doi.org/10.1111/j.1530-0277.2008.00796.x.
Hennen, E. M./Uppuganti, S./Visitación, N. de la/Chen, W./Krishnan, J./Vecchi, L. A./Patrick, D. M./Siedlinski, M./Lemoli, M./Delgado, R./Caestecker, M. P. de/Chang, W./Guzik, T. J./Johnson, R. W./Harrison, D. G./Nyman, J. S. (2025). Hypertension promotes bone loss and fragility by favoring bone resorption in mouse models. The Journal of Clinical Investigation 135 (20). https://doi.org/10.1172/JCI184325.
Holmannova, D./Borsky, P./Kremlacek, J./Krejsek, J./Hodacova, L./Cizkova, A./Fiala, Z./Borska, L. (2025). High prevalence of low vitamin D status in the Czech Republic: a retrospective study of 119,925 participants. European Journal of Clinical Nutrition 79 (7), 641–652. https://doi.org/10.1038/s41430-025-01587-0.
Lee, J. J./Patel, R./Biermann, J. S./Dougherty, P. J. (2013). The Musculoskeletal Effects of Cigarette Smoking. Journal of Bone and Joint Surgery 95 (9), 850–859. https://doi.org/10.2106/jbjs.l.00375.
Lips, P./Cashman, K. D./Lamberg-Allardt, C./Bischoff-Ferrari, H. A./Obermayer-Pietsch, B./Bianchi, M. L./Stepan, J./El-Hajj Fuleihan, G./Bouillon, R. (2019). Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: a position statement of the European Calcified Tissue Society. European Journal of Endocrinology 180 (4), P23-P54. https://doi.org/10.1530/EJE-18-0736.
Lohman, Timothy G./Roche, Alexander F./Martorell, Reynaldo (Eds.) (1988). Anthropometric standardization reference manual. Champaign, Illinois, Human Kinetics Books.
Maskell, P. D./Jones, A. W./Heymsfield, S. B./Shapses, S./Johnston, A. (2020). Total body water is the preferred method to use in forensic blood-alcohol calculations rather than ethanol’s volume of distribution. Forensic Science International 316, 110532. https://doi.org/10.1016/j.forsciint.2020.110532.
Maurel, D. B./Boisseau, N./Benhamou, C. L./Jaffre, C. (2012). Alcohol and bone: review of dose effects and mechanisms. Osteoporosis International 23 (1), 1–16. https://doi.org/10.1007/s00198-011-1787-7.
Mertens, E./Kuijsten, A./Dofková, M./Mistura, L./D'Addezio, L./Turrini, A./Dubuisson, C./Favret, S./Havard, S./Trolle, E./Van't Veer, P./Geleijnse, J. M. (2019). Geographic and socioeconomic diversity of food and nutrient intakes: a comparison of four European countries. European Journal of Nutrition 58 (4), 1475–1493. https://doi.org/10.1007/s00394-018-1673-6.
Natukunda, E./Szubert, A. J./Bamford, A./Doerholt, K./Gibb, D. M./Wandera, C./Nakalyango, A./Griffiths, A./Monkiewicz, L./Nangiya, J. J./Nambi, E./Musiime, V./Musoke, P. (2025). Comparison between dual energy X-ray absorptiometry and calcaneal quantitative ultrasound for determining bone mineral density in children living with HIV in uganda: A cross- sectional study. BMC Pediatrics 25 (1), 529. https://doi.org/10.1186/s12887-025-05881-5.
Nicholson, W. K./Silverstein, M./Wong, J. B./Chelmow, D./Coker, T. R./Davis, E. M./Jaén, C. R./Krousel-Wood, M./Lee, S./Li, L./Mangione, C. M./Ogedegbe, G./Rao, G./Ruiz, J. M./Stevermer, J./Tsevat, J./Underwood, S. M./Wiehe, S. (2025). Screening for Osteoporosis to Prevent Fractures: US Preventive Services Task Force Recommendation Statement. JAMA 333 (6), 498–508. https://doi.org/10.1001/jama.2024.27154.
Popova, S./Rehm, J./Patra, J./Zatonski, W. (2007). Comparing alcohol consumption in central and eastern Europe to other European countries. Alcohol and Alcoholism 42 (5), 465–473. https://doi.org/10.1093/alcalc/agl124.
Puranda, J. L./Edwards, C. M./Weber, V. M. R./Aboudlal, M./Semeniuk, K./Adamo, K. B. (2025). Validity of an ultrasound device to measure bone mineral density. Clinical Anatomy 38 (1), 54–62. https://doi.org/10.1002/ca.24187.
Ratajczak, A. E./Szymczak-Tomczak, A./Rychter, A. M./Zawada, A./Dobrowolska, A./Krela-Kaźmierczak, I. (2021). Impact of Cigarette Smoking on the Risk of Osteoporosis in Inflammatory Bowel Diseases. Journal of Clinical Medicine 10 (7), 1515. https://doi.org/10.3390/jcm10071515.
Sampson, H. W./Perks, N./Champney, T. H./DeFee, B. (1996). Alcohol consumption inhibits bone growth and development in young actively growing rats. Alcoholism: Clinical and Experimental Research 20 (8), 1375–1384. https://doi.org/10.1111/j.1530-0277.1996.tb01137.x.
Sebekova, K./Krivosikova, Z./Gajdos, M./Podracka, L. (2016). Vitamin D status in apparently healthy medication-free Slovaks: Association to blood pressure, body mass index, self-reported smoking status and physical activity. Bratislavske Lekarske Listy 117 (12), 702–709. https://doi.org/10.4149/BLL_2016_135.
Shahbaz, Y./Shirmohammadi, R./Shamsghahfarokhi, S./Esfahani, H./Forghan, M./Eghbali Jelodar, H./Ashrafi, L./Mousavi, M. (2025). Inflammatory impact of cigarette smoking on bone function and structure; a review of evidence. Journal of Parathyroid Disease 13, e13302. https://doi.org/10.34172/jpd.2025.13302.
Soyka, L. A./Fairfield, W. P./Klibanski, A. (2000). Clinical review 117: Hormonal determinants and disorders of peak bone mass in children. The Journal of Clinical Endocrinology and Metabolism 85 (11), 3951–3963. https://doi.org/10.1210/jcem.85.11.6994.
Sripanyakorn, S./Jugdaohsingh, R./Mander, A./Davidson, S. L./Thompson, R. P./Powell, J. J. (2009). Moderate ingestion of alcohol is associated with acute ethanol-induced suppression of circulating CTX in a PTH-independent fashion. Journal of Bone and Mineral Research 24 (8), 1380–1388. https://doi.org/10.1359/jbmr.090222.
Stefler, D./Pajak, A./Malyutina, S./Kubinova, R./Bobak, M./Brunner, E. J. (2016). Comparison of food and nutrient intakes between cohorts of the HAPIEE and Whitehall II studies. European Journal of Public Health 26 (4), 628–634. https://doi.org/10.1093/eurpub/ckv216.
Swinton, P. A./Elliott-Sale, K. J./Sale, C. (2023). Comparative analysis of bone outcomes between quantitative ultrasound and dual-energy x-ray absorptiometry from the UK Biobank cohort. Archives of Osteoporosis 18 (1), 77. https://doi.org/10.1007/s11657-023-01287-x.
Taes, Y./Lapauw, B./Vanbillemont, G./Bogaert, V./Bacquer, D. de/Goemaere, S./Zmierczak, H./Kaufman, J.-M. (2010). Early smoking is associated with peak bone mass and prevalent fractures in young, healthy men. Journal of Bone and Mineral Research 25 (2), 379–387. https://doi.org/10.1359/jbmr.090809.
Tajaldeen, A./Alghamdi, S. S./Aljondi, R./Awan, Z./Helmi, N./Lingawi, K./Mujalad, A./Alzahrani, W. (2022). Associations between body mass index, body composition and bone density in young adults: Findings from Saudi cohort. Journal of Radiation Research and Applied Sciences 15 (1), 268–274. https://doi.org/10.1016/j.jrras.2022.03.010.
Textor, J./van der Zander, B./Gilthorpe, M. S./Liskiewicz, M./Ellison, G. T. (2016). Robust causal inference using directed acyclic graphs: the R package 'dagitty'. International Journal of Epidemiology 45 (6), 1887–1894. https://doi.org/10.1093/ije/dyw341.
Tsao, H. M./Huang, M.-C./Liu, T.-H./Chang, H.-M./Chung, R.-H./Kuo, H.-W./Chen, A. C. H./Yang, R.-S./Liu, Y.-L. (2024). Association of bone turnover markers and craving reduction in patients with alcohol use disorder during withdrawal: Exploring the role of bone-brain axis. Alcohol, Clinical & Experimental Research 48 (12), 2294–2302. https://doi.org/10.1111/acer.15472.
Wang, Q./Nicholson, P. H. F./Timonen, J./Alen, M./Moilanen, P./Suominen, H./Cheng, S. (2008). Monitoring bone growth using quantitative ultrasound in comparison with DXA and pQCT. Journal of Clinical Densitometry 11 (2), 295–301. https://doi.org/10.1016/j.jocd.2007.10.003.
Ward, K. D./Klesges, R. C. (2001). A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcified Tissue International 68 (5), 259–270. https://doi.org/10.1007/bf02390832.
Weng, W./Li, H./Zhu, S. (2022). An Overlooked Bone Metabolic Disorder: Cigarette Smoking-Induced Osteoporosis. Genes 13 (5), 806. https://doi.org/10.3390/genes13050806.
Xie, G./Huang, C./Jiang, S./Li, H./Gao, Y./Zhang, T./Zhang, Q./Volotovski, P./Rahmati, M./Li, Y. (2024). Smoking and osteoimmunology: Understanding the interplay between bone metabolism and immune homeostasis. Journal of Orthopaedic Translation 46, 33–45. https://doi.org/10.1016/j.jot.2024.04.003.
Zhang, W./Wang, X./Liu, Y./He, Q./Ding, Q./Mei, J./Li, X. (2024). Effects of exercise on bone mass and bone metabolism in adolescents: a systematic review and meta-analysis. Frontiers in Physiology 15, 1512822. https://doi.org/10.3389/fphys.2024.1512822.
 ✉
✉