Effect of body composition in the
assessment of growth of Sri Lankan children and need for local
references
Vithanage Pujitha Wickramasinghe ✉
✉
Department of Paediatrics, Faculty of Medicine, University of Colombo, Sri
Lanka
DOI: https://doi.org/10.52905/hbph2022.3.35
Abstract
Measuring growth provides the opportunity to assess an individual’s health and
nutritional status as well as reflect the quality of life and social wellbeing. Global
standards and references for child and adolescent growth have been adopted by many
countries including Sri Lanka, but it is questionable whether these charts are
appropriate. They are known to over-diagnose undernutrition and under-diagnose
over-nutrition in many low-and-middle-income countries.
This article reviews the effect of body composition and ethnicity on the assessment of
growth of Sri Lankan children.
Growth has been documented since early civilization. Standards and references for
assessing intrauterine, infant, child and adolescent growth have evolved for regional,
national, and international use. Attention has been focused on socio-economic, political,
and emotional (SEPE) factors as primary determinants of growth as well as ethnicity.
Growth charts are based on the distribution of growth parameters in the population.
Cut-off values are defined by statistical distributions rather than by the biological
meaning of growth measurements. As most of the adverse health outcomes are related to an
individual’s body composition, anthropometry should correctly reflect body composition and
critical cut-off values should help assessing health risks. Yet, the distributions of
height, weight, and BMI of healthy children of many low-and-middle-income countries
differs from the global growth standards recommended for use by the WHO, and Sri Lankan
children differ and show a shift to the left. In 5- to 15-year-old healthy children
height, weight, and BMI range between -3SD and +1SD. Thus, applying global standards will
often lead to false estimates when defining stunting, thinness, and obesity in these
children. This highlights the importance of local rather than universal growth standards.
Many countries have meanwhile taken the initiative to develop national growth charts.
Further, Sri Lanka needs local growth charts and relevant cut-off values for the correct
assessment of height, weight and BMI.
Keywords: assessment of growth, children, Sri Lanka, body composition and anthropometry, growth charts
Conflict of interest: There are no
conflicts of interest.
Citation: Wickramasinghe, V. (2022). Effect of body composition in the
assessment of growth of Sri Lankan children and need for local
references. Human Biology and Public Health 3. https://doi.org/10.52905/hbph2022.3.35.
Copyright: This is an open access article distributed under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22-05-2022 | Accepted: 12-12-2022 | Published: 10-03-2023
Take-home message for students
It is important to develop appropriate cut-off values for the assessment of height,
weight, and BMI for Sri Lankan children.
Contents
Introduction
Physical growth is a quantitative increase in body size or mass (Bogin 2020). Measurements of growth parameters provide the opportunity
to assess an individual’s health and nutritional status as well as reflect the quality of
life and social wellbeing. Sri Lanka as a middle-income country has shown high achievements
in health indices. However, the anthropometric parameters have not improved beyond a certain
point over a long period of time and since then have stagnated. The last demographic and
health survey (2016) showed stunting (height-for-age) to be 17%, underweight
(weight-for-age) to be 21% and wasting (weight-for-height) to be 15% (Department of Census and Statistics, Ministry of National Policies and
Economic Affairs 2017). This has puzzled health authorities as well as growth
physiologists because of the lack of improvement beyond this point. Many nutrition
supplementation programs as well as awareness programs are being conducted to improve these
indices in Sri Lanka, but with little success. The reasons for the poor improvement of the
nutritional anthropometric indicators have been discussed at many forums, but a proper
explanation has not been found. Apart from stunting, overweight and obesity (OW/OB) among
children and adults are also increasing in the country as well as its related
non-communicable disease (NCD) burden. Doubts have been cast over the use of current
anthropometric indices for the diagnosis of OW/OB due to the increasing case load of NCD
among metabolically unhealthy non-obese individuals (Wickramasinghe et al. 2013).
Growth assessment is mainly based on anthropometric measurements. However, a stand-alone
measurement value is meaningless until it is properly interpreted. Therefore, all
anthropometric measurements should be plotted on the appropriate growth charts. The outcome
of the interpretation then needs to be addressed and actions should be taken.
The evolution of the Assessment of Growth
Since the early civilizations, body proportions were appreciated with careful measurements
of the body at different ages. This is evident in art work, paintings and sculptures (Bogin 2020). Egyptians used a grid system to record body
proportions with the help of which they were even able to accurately demonstrate growth
disorders. Different stages of life were identified by ancient civilizations. Romans
described “seven stages of life” paving the way for current life cycle approaches to an
organism’s biological development (Bogin 2020). In
the 18th century, the interest in studying human growth grew in Europe and the
value of collecting data was appreciated. The French Count Philibert Guéneau du Montbeillard
(1720–1785) collected longitudinal data of his son born in 1759, at six-monthly intervals
until 18 years of age. This is considered the first longitudinal set of human growth data
and was published by George-Louie Leclerc de Buffon (1707–1788) in 1777 in the
Histoire Naturelle (Bogin 2020).
Afterwards, more and more people got interested. Tanner used these data to describe both
distance charts (size) and velocity charts (growth rates).
Differential seasonal variations of height and weight, mid upper arm circumference and
ponderal index were described in Europe during the 19th century. Rudolfo Livi
defined the ponderal index and Quetelet described the BMI (Bogin 2020). In the second half of the 19th century, Henry Bowditch
gathered height and weight measurements from about twenty-four thousand school children and
for the first time constructed percentile growth charts (Bowditch 1891).
During the early 20th century, many longitudinal cohort studies on growth were
started in United States and Europe. The Fels Longitudinal Study in Yellow Springs, Ohio,
from 1929 to 1970 is one of the earliest and most comprehensive studies. The director of the
study, Lester W. Sontag (1901–1991), wrote “… that modern understanding of the growth,
health, behavior, and effectiveness of human beings could only be understood if the nature
and significance of individual characteristics of each child’s physiological, biochemical,
nutritional, educational, and environmental characteristics could be assessed and integrated
into a total picture” (Sontag 1971). As the need
for growth assessment gained importance, Howard Meredith was invited to develop a “Physical
Growth Record” in 1947 (Meredith 1949). It included
charts for assessing weight and height from 4 to 11 years for boys and girls based on
affluent school children from Iowa, USA, in the 1940s (Meredith 1949). In the 1960s and 1970s, this study was followed by several
European and US American growth charts, of which the Tanner (Tanner et al. 1966) and the Harvard growth charts (Stevenson and Stuart 1950) may explicitly been
mentioned. Based on data collected in the Boston region from 1930 to 1956, sex combined
Harvard curves were developed. The WHO used these growth curves later as an international
reference (Jelliffe 1966). The US National Academy
of Sciences recommended a new set of growth references in 1974 based on cross-sectional data
from the US health and examination surveys of the National Centre for Health Statistics
(NCHS) and longitudinal data from the Fels Research Institute (Hegsted et al. 1974). The NCHS and CDC joint expert group developed
growth charts from birth to 18 years of age (head circumference charts for younger ages and
height and weight charts for all ages) (Hamill et al.
1977; Hamill et al. 1979). References for
under 2 years of age were developed using reference data produced by the Fels longitudinal
study collected from 1929 to 1975 from a selected population in Ohio. Data of 2- to
18-year-old children were cross-sectionally collected in three country-wide surveys carried
out in the USA by the NCHS from 1960 to 1975.
In 1975, the WHO recommended to use height and weight reference charts for nutritional
surveillance (Waterlow et al. 1977). Countries that
did not have local reference charts were advised to create local sets of cross-sectional
data. It was recommended to measure at least 200 well-nourished children in each age and sex
group and to perform measurements by trained staff using calibrated equipment (Waterlow et al. 1977). Although all of these criteria
were not met, new US growth references were published by the National Academy of Science
(Hegsted et al. 1974). British references were
published by Tanner et al. (1966) and Dutch references by van
Wieringen (1972). Nevertheless, the WHO
continued to consider the NCHS/CDC charts as the most suitable for international use. Sri
Lanka began to use this sex combined, WHO recommended NCHS/CDC weight-for-age chart from
birth to 5 years of age for the assessment of weight (growth).
The main limitations of these charts were their confinement to an affluent white Caucasian
population and that they were collected at diverse time periods, from predominantly formula
fed children who started with complementary food at different ages. In 1970, Gairdner and
Pearson revised the Tanner charts in the UK (Gairdner, D.,
Pearson, J. 1985). The 1990 growth references of the UK replaced all previous
charts (Cole 1997). The NCHS/CDC 2000 charts
replaced previous charts in the USA (Kuczmarski et al.
2000).
In these years, the variety of European and US American growth charts appeared
disadvantageous and a need for an internationally applicable growth standard was discussed
to better compare the nutritional status of children across the world. It was stated that
height and weight of well-fed healthy children from different ethnic groups and continents
showed only little variation in growth. This notion paved the way for the WHO to consider
international growth standards based on healthy children raised under most suitable
conditions. Such standards were considered to reflect optimum growth in various parts of the
world. In 1996, representative samples from USA, Brazil, Oman, India, Ghana and Norway were
selected and longitudinally followed up from birth to 24 months of life. Cross-sectional
data were added for the ages 25 to 60 months (Borghi
et al. 2006). Smoothed height and BMI-for-age growth charts for children and
adolescents of both sexes aged 5 to 18 years were developed by WHO based on the 1977 NCHS
data (Onis et al. 2007).
In line with adult BMI cut-off values of 25kg/m2, and 30kg/m2 for
overweight and obesity respectively, the International Obesity Task Force developed sex
specific cut-off values at six-monthly intervals for 2- to 18-year old children (Cole et al. 2000). Subsequently, BMI cut-off values to
also diagnose three levels of thinness corresponding to adult BMI values of
16kg/m2, 17kg/m2 and 18.5kg/m2 were added (Cole et al. 2007).
The assessment of growth in Sri Lankan children spans several decades, and it was mostly
done using WHO recommended standards. Island wide uniform growth monitoring began in the
1970s with a weight-for-age chart without sex discrimination. The 50th centile
for boys and 3rd centile for girls up to 5 years of age were based on WHO/NCHS
standards. It aimed at detecting under-nutrition rather than over-nutrition. With the
development of WHO 2006 standard, Sri Lanka incorporated the weight-for-age and
length/height-for-age charts of each sex based on SD scores for under 5 growth monitoring.
Head circumferences for age charts based on centiles from birth to 3 years of age also
included. For children above 5 years, sex specific WHO/NCHS references were used with
height-for-age charts for 5 to 11 years of age and weight-for-height charts for those who
were 90 to 145cm in height. In 2014, above 5-year growth charts were replaced with
height-for-age and BMI-for-age charts for monitoring of growth in 5- to 18-year-old children
for each sex based on WHO 2007 references. In 2019, the centile values for occipital frontal
circumference/head circumference for age was replaced by SD score.
Advances in neonatal care enabled many preterm babies to survive and grow, but the
available infant growth charts were inappropriate for these babies. With an increased
understanding of the impact of early growth on later health and the impact of the first 1000
days of life, growth monitoring during early days became important in the management of
preterm infants. Barker’s hypothesis on the fetal origin of adult disease describes the
association between adverse fetal environment and the prevalence of non-communicable disease
in adulthood (Barker et al. 1993; Barker and Osmond 1986; Barker et al. 1989). The “accelerated growth hypothesis” by Singhal and Lucas
postulates that rapid excess growth during first year of life can lead to adverse health
outcomes later (Singhal et al. 2007). The concept
highlighted the importance of close monitoring of preterm growth in order to prevent the
development of NCD later in life. Using North American data, Babson and Benda developed
graphs for the assessment of preterm infants from 26 weeks of gestation till one year of age
post term (Babson and Benda 1976). These were
updated in 2003 extending to the age from 22 to 50 weeks of gestational age (Fenton 2003).
Nutrition, maternal and fetal disease, intra- as well as extra-uterine environment, and the
genetic potential affect fetal growth and contribute to the differences in birth weights
world-wide. Most of the prenatal growth references were developed on small samples of local
populations. The INTERGROWTH-21st (Villar
et al. 2014) project aimed at assessing fetal growth and newborn size using an
international representative sample. Pregnant women from Brazil, Italy, Oman, UK, and USA,
China, India and Kenya were recruited for a multi-center fetal growth study. This study
showed similar fetal growth and birth size in the different geographical settings as long as
mothers’ nutrition and health are at a high level with minimum environmental constraints.
Combining these data with the WHO growth standards allow for international standards from
conception to birth including the assessment of preterm babies up to 6 months of post term
age. Sri Lanka uses these preterm charts since 2017.
Yet, recent evidence suggests that prenatal growth of Indian children and gestational
weight gain (GWG) which is the proxy measure of intrauterine growth differs from the
INTERGROWTH-21st reference (Thiruvengadam
et al. 2022). 26% of the mothers had a GWG <10th centile at 18-20
weeks, and 45% at time of delivery. Ethnic differences in GWG should be considered when
making clinical decision (Hermanussen 2022).
Reference selection and application
Growth references are statistical summaries of anthropometry, conditioned (usually) on age
and sex. References describe how children do grow, in contrast to growth standards that
prescribe how children should grow (Khadilkar and
Khadilkar 2011). References are descriptive and show how the children are growing
according to their prevailing situation. References relate health, nutrition, and the
social-economic-political-emotional situation to the reference population (Bogin 2021). International charts help to compare
between different countries, socio-economic and ethnic groups, but they may over-report
stunting, wasting, and underweight in many developing countries such as Sri Lanka.
It is important to consider that stunting is not a synonym of malnutrition (Scheffler et al. 2020). Thus, growth references and
standards must not be used to define malnutrition (Bhutta
et al. 2017; Bogin et al. 2022; Hermanussen and Wit 2017; Mumm et al. 2017). This also applies for the population of Sri Lanka.
If we want to focus on malnutrition, it is important to stress that assessing an
individual’s health status needs specific information on nutrition. This includes
information on food availability, on diet diversity, and also on body composition and
measurements of body fat. The diagnosis of malnutrition cannot be based on a single
anthropometric measure (Lara-Pompa et al. 2020). It
should be noted that during the initial stages of life body weight often increases rapidly
with notable upward crossings of several centiles. This does not necessarily reflect
pathological weight gain and later risk of obesity but may rather be part of a proportionate
increase of weight and height to find the correct “growth channel” particularly in children
with low birth weight. Therefore, looking at the broader picture is more important rather
than drawing conclusions on limited number of anthropometric measures.
Population specific growth charts are appropriate instruments for screening and diagnosing
growth impairments which under certain circumstances may also reflect the nutritional
status. However, this is not easy and quite an ardent and costly task for many developing
countries (Sullivan et al. 1991). Population
specific growth charts have synthetically been developed in various countries, e.g. for
Romanian (Pascanu et al. 2016) and Indonesian
children (Pulungan et al. 2018).
The effect of ethnicity on growth assessment
A study done in 2009 in India involving 2 to 5 year old children from affluent families
showed mean SD scores for height, weight, and weight-for-height of -0.75 (SD 1.1), -0.59 (SD
1.1), and -0.26 (SD 1.18), respectively according to WHO 2006 standards (Khadilkar et al. 2010). Mean BMI for age SD score was
–0.19 (SD 1.22). Indonesian children under 5 years have mean height SDS of boys of -2.03 and
of girls of -2.03 when referred to WHO standards (Novina
et al. 2020). This gives food for thought whether growth of even the most affluent
children can be assessed by growth charts developed in other countries or ethnic groups.
Doing so can lead to over-reporting of undernutrition and underreporting of over-nutrition
and in consequence to overtreatment of the undernourished, whereas the metabolic problems of
the over-nourished get under-diagnosed followed by delayed management. Mismatched growth
charts with cut-off values made for Western populations may well have contributed to the
increase in non-communicable disease burden in South Asia.
Growth charts should assist parents and health care workers in guiding a child to achieve
optimum growth. Appropriate growth references are needed as individual health management and
public health decisions rely on them. Appropriate references reflect height, weight, and
body composition of a healthy local population and cut-off values above and below the
‘healthy’ range that appropriately reflect the risks for impaired performance, disease,
morbidity, and mortality. Anthropometry has its place as a valuable screening tool. But it
is not a diagnostic tool for malnutrition. Anthropometry needs to be assessed in combination
with many other factors. Anthropometric charts need to be based on the population
distribution of the various parameters of interest. Single parameters do not always depict
relevant information on morbidity and may lead to serious misclassification of risk factors
for the single individual. This is especially true for children classified as undernourished
though being active and healthy, and with good school performance (Hermanussen 2015; Scheffler et al.
2020).
Body composition as a proxy for nutritional status and health
Body composition is an important factor that is associated with morbidity (Wickramasinghe et al. 2017a). Commonly used parameters
for addressing body composition are height, weight, weight-for-height (under 5 years of
age), and BMI (over 5 years of age).
Body composition of South Asian populations differs from other ethnic groups of the world,
independent of where they live. This is also true for migrants. The BMI for a given fat mass
of South Asian children from Coventry, UK, is lower than the BMI of white children with the
same body fat mass (Eyre et al. 2017). Sri Lankan
children have a higher body fat content compared to their Western counterparts living in
Australia for any given BMI SD score (Wickramasinghe
2011). Sri Lankan children living in their native country have significantly higher
fat mass compared to Australian children of Sri Lankan (migrant) and European origin (Figure 1). Further studies showed that the differences in
body composition between white Europeans and South Asian adults are apparent from early
infancy (Deurenberg et al. 1998; Nightingale et al. 2011; Nightingale et al. 2013). The data suggest that not only genetics, but
also the socio-economic state affect body composition and might explain the low efficacy of
currently used anthropometric cut-off values for Sri Lankan children (Wickramasinghe et al. 2009). The differences in body composition showed
that ethnicity specific body composition prediction equations are needed (Hussain et al. 2014; Nightingale et al. 2013; Wickramasinghe et al.
2005a). The UK CHASE study showed that UK South Asian children are more obese
whereas African Caribbeans are less obese than white Europeans (Nightingale et al. 2011). The body fat content is not well represented
by the BMI and stresses that BMI cut-off points need to be ethnicity specific (Eyre et al. 2017). The manifestation of obesity may be
of genetic origin (Stanfield et al. 2012) or due to
social-economic-political-emotional (SEPE) factors (Bogin
et al. 2022; Wickramasinghe et al.
2009).
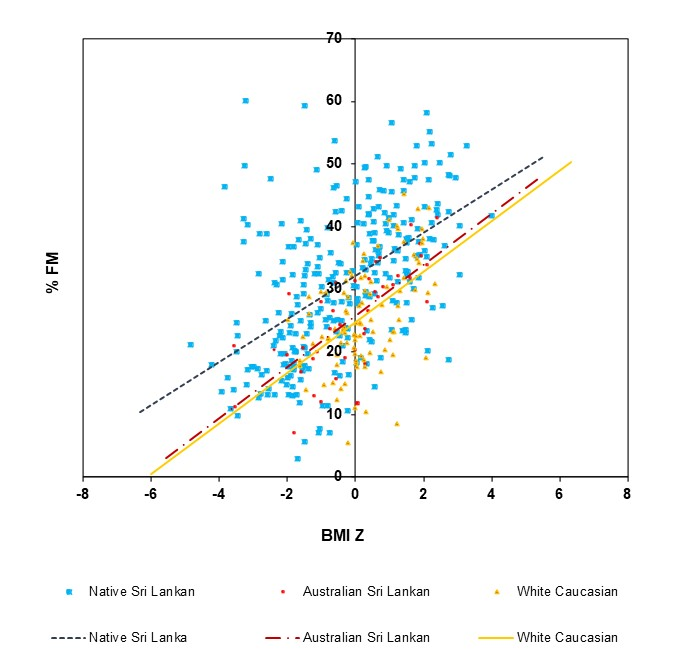
Figure 1 Effect of ethnicity and socioeconomic status on body fat mass of Australian and Sri
Lankan children
Current BMI cut-off values of 5- to 15-year old children have poor sensitivity for
diagnosing obesity in Australian children of Sri Lankan (migrants) and European origin
(Wickramasinghe et al. 2005b), as well as native
Sri Lankan children (Wickramasinghe et al. 2008).
Hattori chart-based analyses of the fat mass distribution of Sri Lankan children shows that
the increase in fat mass is out of proportion to the increase in fat free mass (Wickramasinghe 2012). When Sri Lankan children grow,
they increase the fat mass more than the fat free mass. Current BMI cut-off values
under-estimate excess fat mass and under-diagnose obesity in Sri Lankan children. Western
studies have shown that the non-communicable disease risk varies between a fat percentage of
20–25% in boys and 25–32% in girls (Dwyer and Blizzard
1996; Lohman 1989; Williams et al. 1992). For Sri Lankan children based on the risk of
developing metabolic syndrome, percentage fat mass was defined to be 28.6% for boys and
33.8% for girls (Wickramasinghe et al. 2017a).
Recent considerations on statistical artefacts when assessing BMI z-scores in short and tall
child populations of various age emphasize that the prevalence of thinness, overweight and
obesity depends on height and age and is particularly affected in the short populations
(Hermanussen et al. 2022). Particularly abdominal
fat is an influential risk factor for obesity related metabolic derangements. Waist
circumference appears to be a suitable measure to identify abdominal obesity and is used by
the International Diabetes Federation as an absolute criterion in the diagnosis of the
metabolic syndrome at all ages (Alberti et al. 2006;
Zimmet et al. 2007). Age, sex and ethnic specific
cut-off values for waist circumference are provided by IDF in the diagnosis of metabolic
syndrome (International Diabetes Federation 2007).
Standardized waist to hip circumferences and waist circumference to height ratios were also
explored. The waist to hip circumference ratio did not show good associations with metabolic
derangements in Sri Lankan children (Silva et al.
2006), whereas the waist circumference to height ratio showed good correlations
(Wickramasinghe et al. 2017b). Cut-off values of
0.5 and 0.45 appear to detect the metabolic syndrome, respectively at least two metabolic
derangements, with high sensitivity and specificity (Wickramasinghe et al. 2017b). Therefore, BMI and the waist circumference to height
ratio can be used as an appropriate screening tool in public health settings, although
assessments of body composition would further improve the evaluation of the nutritional
status.
The assessment of growth in Sri Lankan children
Growth monitoring has been an integral part of maternal and child health programs of Sri
Lanka. Up to 5 years of age, growth parameters are usually monitored either at Medical
Officer of Health (MOH) clinics or at mobile weighing posts. The practice is to measure
weight every month till the completion of 2 years and at three-monthly intervals thereafter
until 5 years of age. During the first year of life, it is recommended to measure length at
4 and 9 months – that is the time of the routine immunization - and at half annual intervals
thereafter. Usually, growth during the first year of life is regularly monitored parallel
with visiting the primary health care facility for routine child vaccination. Mobile
weighing posts in the community have additionally increased the compliance for growth
monitoring, with trained volunteers assisting the public health midwives and inviting
parents to bring their children on a routine schedule. Weight-for-length/height is plotted
at six-monthly intervals. Attention should be paid to centile crossings of
weight-for-length/height, not to overlook under- and overweight/obesity.
Growth monitoring in Sri Lanka identified many children with growth faltering at an early
age, particularly infants between 4 and 6 months, and allowed for complimentary feeding
already before 6 months of age. Growth monitoring makes even parents aware of growth
deviations and let them seek medical advice. Yet, it should be stressed that currently
recommended cut-off levels of less than -2SD for height-, weight- and BMI-for-age are
statistical definitions and may not be mistaken as relevant indicators of malnutrition in
the child population of Sri Lanka. The distributions of height, weight and BMI of healthy
Sri Lankan children show a shift to the left when compared with WHO standards. Wickramasinghe and Samaranayake (2016) showed in 5- to 15-year-old healthy children that these
parameters ranged between -3SD and +1SD. Thus, applying WHO standards often leads to false
estimates when defining stunting, thinness, and obesity in these children and highlights the
necessity for local growth references.
We advise to measure weight of school children at least once in 3 months and height at
least once in 6 months. Formal programs occur at school medical inspections at grades 1 (5
years of age), 4 (8 years of age) and 7 (11 years of age). The primary and secondary school
curriculum enforces growth monitoring. Children above the age of 10 years (secondary school)
are empowered to monitor height, weight, and BMI and to have these data plotted and
interpreted on relevant growth charts. Secondary school children are also empowered to
correctly measure their waist circumference as an indicator of abdominal obesity. This has
eliminated the need for calculating the BMI. A waist circumference-to-height ratio of
<0.5 is considered normal.
Local standards are necessary
The Indian Academy of Paediatrics updated its national growth charts in 2021 based on new
representative growth data from the whole of India (Khadikar et al. 2021). Growth of Asian children differs from that of children of
European origin (El-Mouzan et al. 2007; Khadikar et al. 2021; Novina et al. 2020; Zong and Li 2013).
Also Sri Lankan children need to have their own growth charts or at least validate the new
Indian growth charts for the assessing growth in 5–18-year old children from Sri Lanka.
References
Alberti, K. G./Zimmet, P./Shaw, J. (2006).
Metabolic syndrome‐a new world-wide definition. A
Consensus Statement from the International Diabetes Federation. Diabetic Medicine 23
(5), 469–480. https://doi.org/10.1111/j.1464-5491.2006.01858.x.
Babson, S. G./Benda, G. I. (1976). Growth graphs
for the clinical assessment of infants of varying gestational age. The Journal of
Pediatrics 89 (5), 814–820. https://doi.org/10.1016/s0022-3476(76)80815-3.
Barker, D. J./Gluckman, P. D./Godfrey, K.
M./Harding, J. E./Owens, J. A./Robinson, J. S. (1993). Fetal nutrition and
cardiovascular disease in adult life. Lancet 341 (8850), 938–941. https://doi.org/10.1016/0140-6736(93)91224-a.
Barker, D. J./Osmond, C. (1986). Infant mortality,
childhood nutrition, and ischaemic heart disease in England and Wales. Lancet 1 (8489),
1077–1081. https://doi.org/10.1016/s0140-6736(86)91340-1.
Barker, D. J./Winter, P. D./Osmond, C./Margetts,
B./Simmonds, S. J. (1989). Weight in infancy and death from ischaemic heart disease.
Lancet 2 (8663), 577–580. https://doi.org/10.1016/s0140-6736(89)90710-1.
Bhutta, Z. A./Berkley, J. A./Bandsma, R. H.
J./Kerac, M./Trehan, I./Briend, A. (2017). Severe childhood malnutrition. Nature Reviews
Disease Primers 3, 17067. https://doi.org/10.1038/nrdp.2017.67.
Bogin, B. (2020). Patterns of Human Growth.
Cambridge University Press.
Bogin, B. (2021).
Social-Economic-Political-Emotional (SEPE) factors regulate human growth. Human Biology
and Public Health 1, 20. https://doi.org/10.52905/hbph.v1.10.
Bogin, B./Hermanussen, M./Scheffler, C. (2022).
Bergmann’s rule is a "just-so" story of human body size. Journal of Physiological
Anthropology 41 (1), 15. https://doi.org/10.1186/s40101-022-00287-z.
Borghi, E./Onis, M. de/Garza, C./Broeck, J. van
den/Frongillo, E. A./Grummer-Strawn, L./Buuren, S. van/Pan, H./Molinari, L./Martorell,
R./Onyango, A. W./Martines, J. C./Group, W. H. O. Multicentre Growth Reference Study
(2006). Construction of the World Health Organization child growth standards: selection
of methods for attained growth curves. Statistics in Medicine 25 (2), 247–265. https://doi.org/10.1002/sim.2227.
Bowditch, H. P. (1891). The growth of children
studied by Galton’s method of percentile grades. Boston.
Cole, T. J. (1997). Growth monitoring with the
British 1990 growth reference. Archives of Disease in Childhood 76 (1), 47–49. https://doi.org/10.1136/adc.76.1.47.
Cole, T. J./Bellizzi, M. C./Flegal, K. M./Dietz,
W. H. (2000). Establishing a standard definition for child overweight and obesity
worldwide: international survey. The BMJ 320 (7244), 1240–1243. https://doi.org/10.1136/bmj.320.7244.1240.
Cole, T. J./Flegal, K. M./Nicholls, D./Jackson, A.
A. (2007). Body mass index cut offs to define thinness in children and adolescents:
international survey. The BMJ 335 (7612), 194. https://doi.org/10.1136/bmj.39238.399444.55.
Department of Census and Statistics, Ministry of
National Policies and Economic Affairs (2017). Sri Lanka demographic and health survey
2016.
Deurenberg, P./Yap, M./van Staveren, W. A. (1998).
Body mass index and percent body fat: a meta analysis among different ethnic groups.
International Journal of Obesity and Related Metabolic Disorders 22 (12), 1164–1171.
https://doi.org/10.1038/sj.ijo.0800741.
Dwyer, T./Blizzard, C. L. (1996). Defining obesity
in children by biological endpoint rather than population distribution. International
Journal of Obesity and Related Metabolic Disorders 20 (5), 472–480. Available online at
https://www.ncbi.nlm.nih.gov/pubmed/8696427.
El-Mouzan, M. I./Al-Herbish, A. S./Al-Salloum, A.
A./Qurachi, M. M./Al-Omar, A. A. (2007). Growth charts for Saudi children and
adolescents. Saudi Medical Journal 28 (10), 1555–1568. Available online at https://www.ncbi.nlm.nih.gov/pubmed/17914520.
Eyre, E. L. J./Duncan, M. J./Nevill, A. (2017).
South Asian children have increased body fat in comparison to white children at the same
body mass index. Children 4 (11). https://doi.org/10.3390/children4110102.
Fenton, T. R. (2003). A new growth chart for
preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC
Pediatrics 3, 13. https://doi.org/10.1186/1471-2431-3-13.
Gairdner, D., Pearson, J. (1985). Revised
Gairdner-Pearson growth charts. Archives of Disease in Childhood 60,
1202–1206.
Hamill, P. V./Drizd, T. A./Johnson, C. L./Reed, R.
B./Roche, A. F. (1977). NCHS growth curves for children birth-18 years. United States.
Vital and Health Statistics Series 11 (165), i-iv, 1-74. Available online at https://www.ncbi.nlm.nih.gov/pubmed/611680.
Hamill, P. V./Drizd, T. A./Johnson, C. L./Reed, R.
B./Roche, A. F./Moore, W. M. (1979). Physical growth: National Center for Health
Statistics percentiles. The American Journal of Clinical Nutrition 32 (3), 607–629.
https://doi.org/10.1093/ajcn/32.3.607.
Hegsted, D. M./Darby, W. J./Filer, L. J.,
Jr./Shank, R. E. (1974). Comparison of body weights and lengths or heights of groups of
children. Nutrition Reviews 32 (9), 284–288. https://doi.org/10.1111/j.1753-4887.1974.tb00977.x.
Hermanussen, M. (2015). Absolute or relative
measures of height and weight? An editorial. European Journal of Clinical Nutrition 69
(6), 647–648. https://doi.org/10.1038/ejcn.2015.70.
Hermanussen, M. (2022). Pregnant women need local
references for gestational weight gain - an editorial. European Journal of Clinical
Nutrition 76 (6), 781–782. https://doi.org/10.1038/s41430-022-01113-6.
Hermanussen, M./Novine, M./Scheffler, C./Groth, D.
(2022). The arithmetic dilemma when defiining thinness, overweight and obesity in
stunted populations. Human Biology and Public Health 1. https://doi.org/10.52905/hbph2022.1.21.
Hermanussen, M./Wit, J. M. (2017). How much
nutrition for how much growth? Hormone Research in Paediatrics 88 (1), 38–45. https://doi.org/10.1159/000454832.
Hussain, Z./Jafar, T./Zaman, M. U./Parveen,
R./Saeed, F. (2014). Correlations of skin fold thickness and validation of prediction
equations using DEXA as the gold standard for estimation of body fat composition in
Pakistani children. BMJ Open 4 (4), e004194. https://doi.org/10.1136/bmjopen-2013-004194.
International Diabetes Federation (2007). The IDF
consensus definition of the metablic syndrome in children and adolescents. Brussels, IDF
Communication.
Jelliffe, D. B. (1966). The assessment of the
nutritional status of the community (with special reference to field surveys in
developing regions of the world). Monograph series. World Health Organization 53, 3–271.
Available online at https://www.ncbi.nlm.nih.gov/pubmed/4960818.
Khadikar, V./Khadilkar, A. V./Lohiya, N.
N./Karguppikar, M. B. (2021). Extended growth charts for Indian children. Journal of
Pediatric Endocrinology and Metabolism 34 (3), 357–362. https://doi.org/10.1515/jpem-2020-0573.
Khadilkar, V. V./Khadilkar, A. V./Chiplonkar, S.
A. (2010). Growth performance of affluent Indian preschool children: a comparison with
the new WHO growth standard. Indian Pediatrics 47 (10), 869–872. https://doi.org/10.1007/s13312-010-0147-6.
Khadilkar, V./Khadilkar, A. (2011). Growth charts:
A diagnostic tool. Indian Journal of Endocrinology and Metabolism 15 Suppl 3, S166-71.
https://doi.org/10.4103/2230-8210.84854.
Kuczmarski, R. J./Ogden, C. L./Grummer-Strawn, L.
M./Flegal, K. M./Guo, S. S./Wei, R./Mei, Z./Curtin, L. R./Roche, A. F./Johnson, C. L.
(2000). CDC growth charts: United States. Advance data from vital and health statistics
(314), 1–27. Available online at https://www.ncbi.nlm.nih.gov/pubmed/11183293.
Lara-Pompa, N. E./Hill, S./Williams, J./Macdonald,
S./Fawbert, K./Valente, J./Kennedy, K./Shaw, V./Wells, J. C./Fewtrell, M. (2020). Use of
standardized body composition measurements and malnutrition screening tools to detect
malnutrition risk and predict clinical outcomes in children with chronic conditions. The
American Journal of Clinical Nutrition 112 (6), 1456–1467. https://doi.org/10.1093/ajcn/nqaa142.
Lohman, T. G. (1989). The prevalence of obesity in
children in the United States. Chmapaign, IL, Human Kinetics, Monogram.
Meredith, H. V. (1949). A physical growth record
for use in elementary and high schools. American Journal of Public Health and the
Nation's Health 39 (7), 878–885. https://doi.org/10.2105/ajph.39.7.878.
Mumm, R./Czernitzki, A. F./Bents, D./Musalek, M.
(2017). Socioeconomic situation and growth in infants and juveniles. Anthropologischer
Anzeiger 74 (2), 101–107. https://doi.org/10.1127/anthranz/2017/0706.
Nightingale, C. M./Rudnicka, A. R./Owen, C.
G./Cook, D. G./Whincup, P. H. (2011). Patterns of body size and adiposity among UK
children of South Asian, black African-Caribbean and white European origin: Child Heart
And health Study in England (CHASE Study). International Journal of Epidemiology 40 (1),
33–44. https://doi.org/10.1093/ije/dyq180.
Nightingale, C. M./Rudnicka, A. R./Owen, C.
G./Donin, A. S./Newton, S. L./Furness, C. A./Howard, E. L./Gillings, R. D./Wells, J.
C./Cook, D. G./Whincup, P. H. (2013). Are ethnic and gender specific equations needed to
derive fat free mass from bioelectrical impedance in children of South asian, black
african-Caribbean and white European origin? Results of the assessment of body
composition in children study. PLoS One 8 (10), e76426. https://doi.org/10.1371/journal.pone.0076426.
Novina, N./Hermanussen, M./Scheffler, C./Pulungan,
A. B./Ismiarto, Y. D./Andriyana, Y./Biben, V./Setiabudiawan, B. (2020). Indonesian
National Growth Reference Charts Better Reflect Height and Weight of Children in West
Java, Indonesia, than WHO Child Growth Standards. Journal of Clinical Research in
Pediatric Endocrinology 12 (4), 410–419. https://doi.org/10.4274/jcrpe.galenos.2020.2020.0044.
Onis, M. de/Onyango, A. W./Borghi, E./Siyam,
A./Nishida, C./Siekmann, J. (2007). Development of a WHO growth reference for
school-aged children and adolescents. Bulletin of the World Health Organization 85 (9),
660–667. https://doi.org/10.2471/blt.07.043497.
Pascanu, I./Pop, R./Barbu, C. G./Dumitrescu, C.
P./Gherlan, I./Marginean, O./Preda, C./Procopiuc, C./Vulpoi, C./Hermanussen, M. (2016).
Development of synthetic growth charts for Romanian population. Acta Endocrinologica 12
(3), 309–318. https://doi.org/10.4183/aeb.2016.309.
Pulungan, A. B./Julia, M./Batubara, J. R.
L./Hermanussen, M. (2018). Indonesian national synthetic growth charts. Acta Scientific
Paediatrics 1 (1), 15. Available online at https://www.actascientific.com/ASPE/pdf/ASPE-01-0006.pdf (accessed
2/3/2023).
Scheffler, C./Hermanussen, M./Bogin, B./Liana, D.
S./Taolin, F./Cempaka, Pmvp/Irawan, M./Ibbibah, L. F./Mappapa, N. K./Payong, M. K.
E./Homalessy, A. V./Takalapeta, A./Apriyanti, S./Manoeroe, M. G./Dupe, F. R./Ratri, R.
R. K./Touw, S. Y./K, P. V./Murtani, B. J./Nunuhitu, R./Puspitasari, R./Riandra, I.
K./Liwan, A. S./Amandari, P./Permatasari, A. A. I./Julia, M./Batubara, J./Pulungan, A.
(2020). Stunting is not a synonym of malnutrition. European Journal of Clinical
Nutrition 74 (3), 377–386. https://doi.org/10.1038/s41430-019-0439-4.
Silva, K. S. de/Wickramasinghe, V. P./Gooneratne,
I. N. (2006). Metabolic consequences of childhood
obesity‐a preliminary report. Ceylon Medical Journal
51 (3), 105–109. https://doi.org/10.4038/cmj.v51i3.1253.
Singhal, A./Cole, T. J./Fewtrell, M./Kennedy,
K./Stephenson, T./Elias-Jones, A./Lucas, A. (2007). Promotion of faster weight gain in
infants born small for gestational age: is there an adverse effect on later blood
pressure? Circulation 115 (2), 213–220. https://doi.org/10.1161/CIRCULATIONAHA.106.617811.
Sontag, L. W. (1971). The history of longitudinal
research: implications for the future. Child Development 42 (4), 987–1002. Available
online at https://www.ncbi.nlm.nih.gov/pubmed/4945427.
Stanfield, K. M./Wells, J. C./Fewtrell, M.
S./Frost, C./Leon, D. A. (2012). Differences in body composition between infants of
South Asian and European ancestry: the London Mother and Baby Study. International
Journal of Epidemiology 41 (5), 1409–1418. https://doi.org/10.1093/ije/dys139.
Stevenson, S. S./Stuart, H. C. (1950). Paranatal
factors affecting adjustment in childhood. American Journal of Diseases of Children 79
(5), 931–934. Available online at https://www.ncbi.nlm.nih.gov/pubmed/15410693.
Sullivan, K./Trowbridge, F./Gorstein, J./Pradilla,
A. (1991). Growth references. Lancet 337 (8754), 1420–1421. https://doi.org/10.1016/0140-6736(91)93113-n.
Tanner, J. M./Whitehouse, R. H./Takaishi, M.
(1966). Standards from birth to maturity for height, weight, height velocity, and weight
velocity: British children, 1965. I. Archives of Disease in Childhood 41 (219), 454–471.
https://doi.org/10.1136/adc.41.219.454.
Thiruvengadam, R./Desiraju, B. K./Natchu, U. C.
M./Wadhwa, N./Sachdeva, K./Misra, S./Parmar, N./Juyal, M./Mittal, P./Bharti,
R./Tripathi, R./Ramji, S./Sachdev, H. S./Bhatnagar, S./GARBH–Ini study team (2022).
Gestational weight gain trajectories in GARBH-Ini pregnancy cohort in North India and a
comparative analysis with global references. European Journal of Clinical Nutrition 76
(6), 855–862. https://doi.org/10.1038/s41430-021-01040-y.
van Wieringen, J. C. (1972). Secular Changes of
Growth. 1964-1966 height and weight surveys in the Netherlands.
Villar, J./Papageorghiou, A. T./Pang, R./Ohuma, E.
O./Cheikh Ismail, L./Barros, F. C./Lambert, A./Carvalho, M./Jaffer, Y. A./Bertino,
E./Gravett, M. G./Altman, D. G./Purwar, M./Frederick, I. O./Noble, J. A./Victora, C.
G./Bhutta, Z. A./Kennedy, S. H./International, Fetal/Newborn Growth Consortium for the
21st, Century (2014). The likeness of fetal growth and newborn size across non-isolated
populations in the INTERGROWTH-21st Project: the Fetal Growth Longitudinal Study and
Newborn Cross-Sectional Study. Lancet Diabetes Endocrinol 2 (10), 781–792. https://doi.org/10.1016/S2213-8587(14)70121-4.
Waterlow, J. C./Buzina, R./Keller, W./Lane, J.
M./Nichaman, M. Z./Tanner, J. M. (1977). The presentation and use of height and weight
data for comparing the nutritional status of groups of children under the age of 10
years. Bulletin of the World Health Organization 55 (4), 489–498. Available online at
https://www.ncbi.nlm.nih.gov/pubmed/304391.
Wickramasinghe, V. P. (2011). Body composition of
Sri Lankan children: Effects of ethnicity. Sri Lanka Journal of Child Health 40 (3),
89–104.
Wickramasinghe, V. P. (2012). Hattori chart based
evaluation of body composition and its relation to body mass index in a group of Sri
Lankan children. Indian Journal of Pediatrics 79 (5), 632–639. https://doi.org/10.1007/s12098-011-0615-6.
Wickramasinghe, V. P./Arambepola, C./Bandara,
P./Abeysekera, M./Kuruppu, S./Dilshan, P./Dissanayake, B. S. (2013). Distribution of
obesity-related metabolic markers among 5-15 year old children from an urban area of Sri
Lanka. Annals of Human Biology 40 (2), 168–174. https://doi.org/10.3109/03014460.2012.753109.
Wickramasinghe, V. P./Arambepola, C./Bandara,
P./Abeysekera, M./Kuruppu, S./Dilshan, P./Dissanayake, B. S. (2017a). Defining obesity
using a biological end point in Sri Lankan children. Indian Journal of Pediatrics 84
(2), 117–123. https://doi.org/10.1007/s12098-016-2191-2.
Wickramasinghe, V. P./Arambepola, C./Bandara,
P./Abeysekera, M./Kuruppu, S./Dilshan, P./Dissanayake, B. S. (2017b). Use of waist to
height ratio in assessing metabolic derangements among normal and overweight/obese 5-15
year old individuals. Ceylon Journal of Medical Sciences 54 (1), 9. https://doi.org/10.4038/cjms.v54i1.4813.
Wickramasinghe, V. P./Cleghorn, G. J./Edmiston, K.
A./Davies, P. S. (2005a). Impact of ethnicity upon body composition assessment in Sri
Lankan Australian children. Journal of Paediatrics and Child Health 41 (3), 101–106.
https://doi.org/10.1111/j.1440-1754.2005.00558.x.
Wickramasinghe, V. P./Cleghorn, G. J./Edmiston, K.
A./Murphy, A. J./Abbott, R. A./Davies, P. S. (2005b). Validity of BMI as a measure of
obesity in Australian white Caucasian and Australian Sri Lankan children. Annals of
Human Biology 32 (1), 60–71. https://doi.org/10.1080/03014460400027805.
Wickramasinghe, V. P./Lamabadusuriya, S.
P./Cleghorn, G. J./Davies, P. S. (2008). Assessment of body composition in Sri Lankan
children: validation of a skin fold thickness equation. Ceylon Medical Journal 53 (3),
83–88. https://doi.org/10.4038/cmj.v53i3.247.
Wickramasinghe, V. P./Lamabadusuriya, S.
P./Cleghorn, G. J./Davies, P. S. (2009). Validity of currently used cutoff values of
body mass index as a measure of obesity in Sri Lankan children. Ceylon Medical Journal
54 (4), 114–119. https://doi.org/10.4038/cmj.v54i4.1451.
Wickramasinghe, V. P./Samaranayake, D. B. (2016).
Growth charts: do they reflect healthy growth in Sri Lankan children? BMC Research Notes
9, 208. https://doi.org/10.1186/s13104-016-2016-4.
Williams, D. P./Going, S. B./Lohman, T. G./Harsha,
D. W./Srinivasan, S. R./Webber, L. S./Berenson, G. S. (1992). Body fatness and risk for
elevated blood pressure, total cholesterol, and serum lipoprotein ratios in children and
adolescents. American Journal of Public Health 82 (3), 358–363. https://doi.org/10.2105/ajph.82.3.358.
Zimmet, P./Alberti, K. G./Kaufman, F./Tajima,
N./Silink, M./Arslanian, S./Wong, G./Bennett, P./Shaw, J./Caprio, S./Group, I. D. F.
Consensus (2007). The metabolic syndrome in children and adolescents - an IDF consensus
report. Pediatric Diabetes 8 (5), 299–306. https://doi.org/10.1111/j.1399-5448.2007.00271.x.
Zong, X. N./Li, H. (2013). Construction of a new
growth references for China based on urban Chinese children: comparison with the WHO
growth standards. PLoS One 8 (3), e59569. https://doi.org/10.1371/journal.pone.0059569.